Most Popular steroids USA
-
 Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00 -
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.
-
Somatrox XT Labs 150 IU x 10 vials (15 ui each)
Original price was: $450.00.$350.00Current price is: $350.00.












Testesterone P 100mg/ml 10ml (Testosterone Propionate) – Medical Pharma
$93.00
C22H32O3 = 344.5.
CAS — 57-85-2.
ATC — G03BA03.
ATC Vet — QG03BA03.
SP 31(Testosterone Propionate). White or creamy-white, odourless, crystals or crystalline powder. Insoluble in water; freely soluble in alcohol, in dioxan, in ether, and in other organic solvents; soluble in vegetable oils. Protect from light.
Testosterone contains: 100mg 100 mg / ml Testosterone Propionate.
Testesterone P 100mg/ml 10ml (Testosterone Propionate) – Medical Pharma Steroid in USA
Testesterone P dosing: Adult
Inoperable metastatic breast cancer (females): IM: 200 to 400 mg every 2 to 4 weeks.
Hypogonadism or hypogonadotropic hypogonadism (males):
IM: 50 to 400 mg every 2 to 4 weeks; 75 to 100 mg/week or 150 to 200 mg every 2 weeks.
Delayed puberty (males):
IM (testosterone enanthate): 50 to 200 mg every 2 to 4 weeks for a limited duration.
Dosing: Geriatric
Refer to adult dosing.
Dosing: Pediatric
Delayed puberty (adolescent males):
IM: Refer to adult dosing.
Hypogonadism or hypogonadotropic hypogonadism (adolescent males):
IM : Refer to adult dosing.
Dosing: Renal impairment
There are no dosage adjustments provided in manufacturer’s labeling (has not been studied). Use with caution; may enhance edema formation. Testosterone propionate is contraindicated in serious renal disease.
Dosing: Hepatic Impairment
There are no dosage adjustments provided in manufacturer’s labeling (has not been studied). Use with caution; may enhance edema formation. Testosterone propionate is contraindicated in serious hepatic disease.
Use: Labeled indications
Injection: Androgen replacement therapy in the treatment of delayed male puberty; male hypogonadism (primary or hypogonadotropic).
Administration: IM
Administer by deep IM injection into the gluteal muscle.
Testosterone propionate: Warm to room temperature; shaking vial will help redissolve crystals that have formed after storage.
Hazardous agent; use appropriate precautions for handling and disposal (NIOSH 2014 [group 3]).
Storage/Stability
Store at room temperature. Protect from light.
Preparation for administration
Injection:
Testosterone propionate: Warm to room temperature; shaking vial will help redissolve crystals that have formed after storage.
Contraindications
Hypersensitivity to testosterone or any component of the formulation; males with carcinoma of the breast or known or suspected carcinoma of the prostate; women who are breast-feeding, pregnant, or who may become pregnant.
Depo-Testosterone: Also contraindicated in serious hepatic, renal, or cardiac disease.
Documentation of allergenic cross-reactivity for androgens is limited. However, because of similarities in chemical structure and/or pharmacologic actions, the possibility of cross-sensitivity cannot be ruled out with certainty.
Warnings/Precautions
Concerns related to adverse effects:
Cardiovascular events: Studies have suggested an increased risk of cardiovascular events among groups of men prescribed testosterone therapy (Basaria, 2010; Finkle, 2014; Vigen, 2013). The Endocrine Society suggests it may be prudent to avoid testosterone therapy in men who have experienced a cardiovascular event (eg, MI, stroke, acute coronary syndrome) in the past six months (The Endocrine Society, 2014). These risks are currently under review by the FDA (Drug Safety Communication, 2014).
Dyslipidemia: May alter serum lipid profile; use caution with history of MI or coronary artery disease.
Gynecomastia: May cause Gynecomastia.
Hepatic effects: Prolonged use of high doses of oral androgens has been associated with serious hepatic effects (peliosis hepatis, hepatic neoplasms, cholestatic hepatitis, jaundice). Prolonged use of intramuscular testosterone enanthate has been associated with multiple hepatic adenomas. Discontinue therapy if signs or symptoms of hepatic dysfunction (such as jaundice) develop.
Hypercalcemia: May cause hypercalcemia in patients with prolonged immobilization or cancer.
Hypoglycemia: May decrease glucose levels.
Polycythemia: May increase hematocrit requiring dose adjustment or discontinuation. Discontinue therapy if hematocrit exceeds 54%; may reinitiate at lower dose (Bhasin, 2010).
Prostate cancer: May increase the risk of prostate cancer.
Spermatogenesis: Large doses may suppress spermatogenesis.
Venous thromboembolism: Venous thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), have been reported with testosterone products. Evaluate patients with symptoms of pain, edema, warmth, and erythema in the lower extremity for DVT and those with acute shortness of breath for PE. Discontinue therapy if a venous thromboembolism is suspected.
Disease related concerns:
Benign prostatic hyperplasia (BPH): Androgens may worsen BPH; patients may also be at an increased risk of prostate cancer. Discontinue therapy if urethral obstruction develops in patients with BPH (use lower dose if restarted). Withhold therapy pending urological evaluation in patients with palpable prostate nodule or induration, PSA >4 ng/mL, or PSA >3 ng/mL in men at high risk of prostate cancer (Bhasin, 2010).
Diseases exacerbated by fluid retention: Use with caution in patients with diseases that may be exacerbated by fluid retention, including cardiac, hepatic, or renal dysfunction; Testosterone may cause fluid retention.
Sleep apnea: May potentiate sleep apnea in some male patients (obesity or chronic lung disease).
Concurrent drug therapy issues:
Drug-drug interactions: Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
Special populations:
Elderly: May be inappropriate in this age group due to potential risk of cardiac problems and contraindication for use in men with prostate cancer; in general, avoid use in older adults except in the setting of moderate-to-severe hypogonadism (Beers Criteria). In addition, elderly patients may be at greater risk for prostatic hyperplasia, prostate cancer, fluid retention, and transaminase elevations.
Pediatric: May accelerate bone maturation without producing compensatory gain in linear growth in children; in prepubertal children perform radiographic examination of the hand and wrist every 6 months to determine the rate of bone maturation and to assess the effect of treatment on the epiphyseal centers. Gels, solution, transdermal, and buccal system have not been evaluated in males <18 years of age; safety and efficacy of injection have not been established in males <12 years of age.
Women: During treatment for metastatic breast cancer, women should be monitored for signs of virilization; discontinue if mild virilization is present to prevent irreversible symptoms.
Dosage form specific issues:
Benzyl alcohol and derivatives: Some dosage forms may contain benzyl alcohol; large amounts of benzyl alcohol (≥99 mg/kg/day) have been associated with a potentially fatal toxicity (“gasping syndrome”) in neonates; the “gasping syndrome” consists of metabolic acidosis, respiratory distress, gasping respirations, CNS dysfunction (including convulsions, intracranial hemorrhage), hypotension, and cardiovascular collapse (AAP, 1997; CDC, 1982); some data suggests that benzoate displaces bilirubin from protein binding sites (Ahlfors, 2001); avoid or use dosage forms containing benzyl alcohol with caution in neonates. See manufacturer’s labeling.
Castor oil: Some products may contain castor oil.
Soy: Some testosterone products may be chemically synthesized from soy.
Special handling:
Hazardous agent: Use appropriate precautions for handling and disposal (NIOSH 2014 [group 3]).
Other warnings/precautions:
Abuse/misuse/diversion: Anabolic steroids may be abused; abuse may be associated with adverse physical and psychological effects.
Geriatric considerations
Elderly males treated with androgens may be at increased risk of developing prostatic hyperplasia and prostatic carcinoma. Increase in libido may occur.
Pregnancy risk factor
X (Contraindicated)
Category X: Studies in animals or human beings have demonstrated fetal abnormalities, or there is evidence of fetal risk based on human experience, or both, and the risk of the use of the drug in pregnant women clearly outweighs any possible benefit. The drug is contraindicated in women who are or may become pregnant.
Pregnancy considerations
Testosterone may cause adverse effects, including masculinization of the female fetus, if used during pregnancy.
Lactation
Enters breast milk – contraindicated in lactation.
Breast feeding considerations
High levels of endogenous maternal testosterone, such as those caused by certain ovarian cysts, suppress milk production. Maternal serum testosterone levels generally fall following pregnancy and return to normal once breast-feeding is stopped. The amount of testosterone present in breast milk or the effect to the nursing infant following maternal supplementation is not known. Some products are contraindicated while breast-feeding.
Adverse reactions
Frequency not always defined.
Cardiovascular: Hypertension (≥3%), increased blood pressure (1%), decreased blood pressure, deep vein thrombosis, edema, vasodilatation.
Central nervous system: Headache (1% to ≥3%), fatigue (2%), irritability (2%), insomnia (≤2%), mood swings (≤2%), aggressive behavior (1%), taste disorder (1%), altered sense of smell (≤1%), abnormal dreams, amnesia, anxiety, chills, depression, dizziness, emotional lability, excitement, hostility, malaise, nervousness, outbursts of anger, paresthesia, seizure, sleep apnea, suicidal ideation
Dermatologic: Acne vulgaris (5%), hyperhidrosis (1%), alopecia, contact dermatitis, diaphoresis, erythema, folliculitis, hair discoloration, pruritus, seborrhea, skin rash, xeroderma.
Endocrine & metabolic: Increased plasma estradiol concentration (3%), weight gain (1%), gynecomastia (≤1%), hot flash (≤1%), change in libido, decreased gonadotropin, fluid retention, hirsutism (increase in pubic hair growth), hypercalcemia, hyperchloremia, hypercholesterolemia, hyperglycemia, hyperkalemia, hyperlipidemia, hypernatremia, hypoglycemia, hypokalemia, inorganic phosphate retention, menstrual disease (including amenorrhea).
Gastrointestinal: Diarrhea (≥3%), gastroesophageal reflux disease, gastrointestinal hemorrhage, gastrointestinal irritation, increased appetite, nausea, vomiting.
Genitourinary: Prostate specific antigen increase (5% to 11%), prostatitis (≥3%), ejaculatory disorder (1%), prostate induration (1%), spontaneous erections (≤1%), benign prostatic hypertrophy, difficulty in micturition, hematuria, impotence, irritable bladder, mastalgia, oligospermia, priapism, testicular atrophy, urinary tract infection, virilization.
Hepatic: Abnormal hepatic function tests, cholestatic hepatitis, cholestatic jaundice, hepatic insufficiency, hepatic necrosis, hepatocellular neoplasms, increased serum bilirubin, peliosis hepatis.
Hematologic & oncologic: Increased hematocrit (1% to 3%), increased hemoglobin (2%), malignant neoplasm of prostate (1%), anemia, clotting factors suppression, hemorrhage, leukopenia, polycythemia, prostate carcinoma.
Hypersensitivity: Anaphylactoid reaction, hypersensitivity reaction (including pulmonary oil microembolism).
Local: Pain at injection site (5%), erythema at injection site (1%), application site reaction (gel, solution), inflammation at injection site
Neuromuscular & skeletal: Arthralgia (≥3%), back pain (≥3%), abnormal bone growth (accelerated), hemarthrosis, hyperkinesia, weakness.
Ophthalmic: Increased lacrimation.
Renal: Increased serum creatinine, polyuria.
Respiratory: Bronchitis (≥3%), nasopharyngitis (≥3%), sinusitis (≥3%), upper respiratory tract infection (≥3%), dyspnea
<1%, postmarketing, and/or case reports: Injection, gel: Abdominal pain, abnormal erythropoiesis, abscess at injection site, allergic dermatitis, anaphylactic shock, anaphylaxis, androgenetic alopecia, angina pectoris, angioedema, asthma, breast induration, cardiac arrest, cardiac failure, cerebral infarction, cerebrovascular accident, cerebrovascular insufficiency, chest pain, chronic obstructive pulmonary disease, circulatory shock, cognitive dysfunction, confusion, coronary artery disease, coronary occlusion, cough, decreased plasma testosterone, decreased thyroxine binding globulin, decreased urinary calcium excretion, diabetes mellitus, dysuria, electrolyte disturbance, epididymitis, erectile dysfunction, hearing loss (sudden), hematoma at injection site, hepatotoxicity (idiosyncratic) (Chalasani, 2014), hyperparathyroidism, hypersensitivity angiitis, hypertriglyceridemia, hyperventilation, impaired glucose tolerance, increased gamma-glutamyl transferase, increased intraocular pressure, increased serum ALT, increased serum AST, increased serum prolactin, increased serum transaminases, increased serum triglycerides, Korsakoff’s psychosis (nonalcoholic), migraine, musculoskeletal chest pain, musculoskeletal pain, myalgia, myocardial infarction, nephrolithiasis, nipple tenderness, orgasm disturbance (male), osteopenia, osteoporosis, peripheral edema, personality disorder, pharyngeal edema, pharyngolaryngeal pain, prolonged partial thromboplastin time, prolonged prothrombin time, prostatic intraepithelial neoplasia, pulmonary embolism, pure red cell aplasia, renal colic, renal pain, respiratory distress, restlessness, reversible ischemic neurological deficit, rhinitis, sleep disorder, snoring, spermatocele, syncope, systemic lupus erythematosus, tachycardia, testicular pain, thrombocytopenia, thromboembolism, thrombosis, tinnitus, transient ischemic attacks, urinary incontinence, urolithiasis, urticaria, venous insufficiency, venous thromboembolism, vesicobullous rash, virilization (of children, following secondary exposure to topical gel [advanced bone age, aggressive behavior, enlargement of clitoris requiring surgery, enlargement of penis, increased erections, increased libido, pubic hair development]), vitreous detachment, voice disorder.
Metabolism/Transport effects
Drug Interactions
Blood Glucose Lowering Agents: Androgens may enhance the hypoglycemic effect of Blood Glucose Lowering Agents. Risk C: Monitor therapy.
C1 inhibitors: Androgens may enhance the thrombogenic effect of C1 inhibitors. Risk C: Monitor therapy.
Corticosteroids (Systemic): May enhance the fluid-retaining effect of Androgens. Risk C: Monitor therapy.
CycloSPORINE (Systemic): Androgens may enhance the hepatotoxic effect of Cyclosporine (Systemic). Androgens may increase the serum concentration of Cyclosporine (Systemic). Risk D: Consider therapy modification.
Dehydroepiandrosterone: May enhance the adverse/toxic effect of Testosterone. Risk X: Avoid combination.
Vitamin K Antagonists (eg, warfarin): Androgens may enhance the anticoagulant effect of Vitamin K Antagonists. Risk D: Consider therapy modification.
Test interactions
Testosterone may decrease thyroxine-binding globulin, resulting in decreased total T4; free thyroid hormone levels are not changed.
Monitoring Parameters.
Periodic liver function tests, lipid panel, hemoglobin and hematocrit (prior to therapy, at 3 to 6 months, then annually); radiologic examination of wrist and hand every 6 months (when using in prepubertal children). Withhold initial treatment with hematocrit >50% (discontinue therapy if hematocrit exceeds 54% [Bhasin, 2010]), hyperviscosity, untreated obstructive sleep apnea, or uncontrolled severe heart failure. Monitor urine and serum calcium and signs of virilization in women treated for breast cancer. Serum glucose (may be decreased by testosterone, monitor patients with diabetes). Evaluate males for response to treatment and adverse events 3 to 6 months after initiation and then annually.
Bone mineral density: Monitor after 1 to 2 years of therapy in hypogonadal men with osteoporosis or low trauma fracture (Bhasin, 2010).
PSA: In men >40 years of age with baseline PSA >0.6 ng/mL, PSA and prostate exam (prior to therapy, at 3 to 6 months, then as based on current guidelines). Withhold treatment pending urological evaluation in patients with palpable prostate nodule or induration or PSA >4 ng/mL or if PSA >3 ng/mL in men at high risk of prostate cancer (Bhasin, 2010).
Do not treat with severe untreated BPH with IPSS symptom score >19.
Serum testosterone: After initial dose titration (if applicable), monitor 3 to 6 months after initiating treatment, then annually.
Injection:
Testosterone enanthate: Measure midway between injections. Adjust dose or frequency if testosterone concentration is <400 ng/dL or >700 ng/dL (Bhasin, 2010).
Testosterone undecanoate: Measure just prior to each subsequent injection and adjust dosing interval to maintain serum testosterone in mid-normal range (Bhasin, 2010).
Reference range
Total testosterone, males:
12 to 13 years: <800 ng/dL
14 years: <1200 ng/dL
15 to 16 years: 100 to 1200 ng/dL
17 to 18 years: 300 to 1200 ng/dL
19 to 40 years: 300 to 950 ng/dL
>40 years: 240 to 950 ng/dL
Free testosterone, males: 9 to 30 ng/dL
Dosage forms
Solution, Intramuscular, as propionate:
10mg/ml, 20mg/ml, 25mg/ml, 50mg/ml, 100mg/ml disolved in oil.
Anatomic Therapeutic Chemical (ATC) Classification.
G03BA03.
Mechanism of action
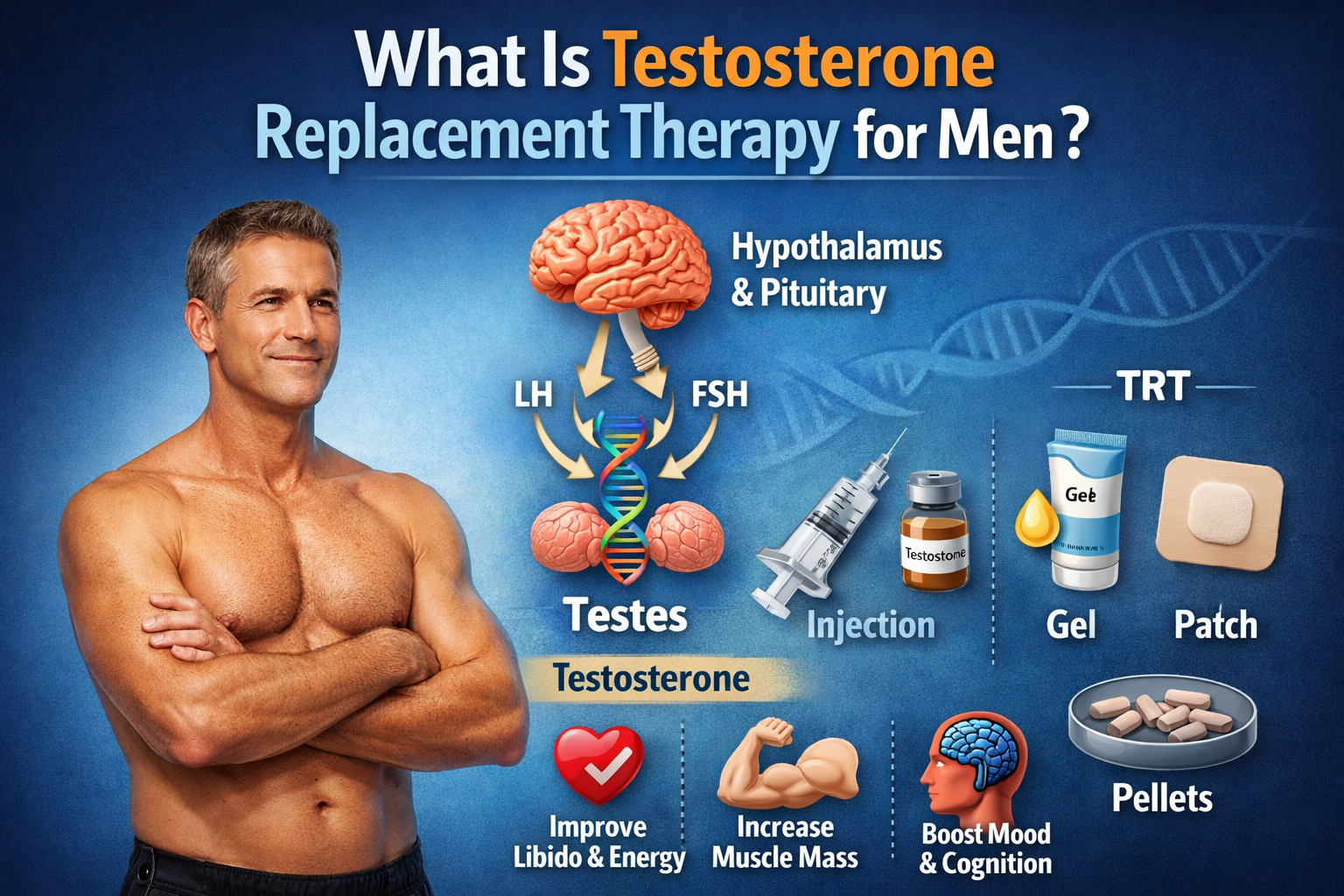
Principal endogenous androgen responsible for promoting the growth and development of the male sex organs and maintaining secondary sex characteristics in androgen-deficient males.
Pharmacodynamics/Kinetics
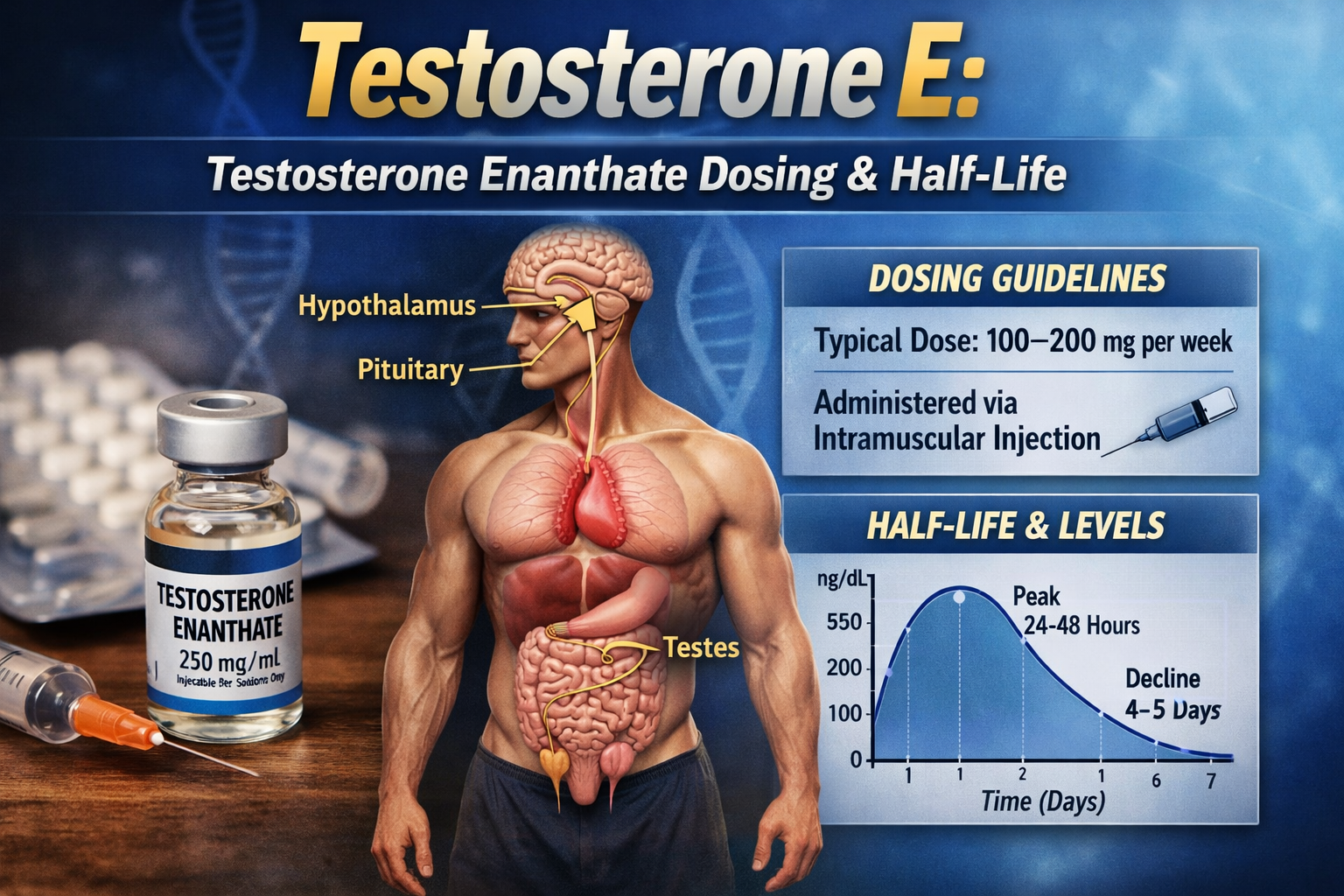
Duration (route and ester dependent): IM: Cypionate and enanthate esters have longest duration, ≤2 to 4 weeks; Undecanoate 10 weeks; Propionate 24-48 hours.
Protein binding: 98%; bound to sex hormone-binding globulin (40%) and albumin.
Metabolism: Hepatic; forms metabolites, including dihydrotestosterone (DHT) and estradiol (both active).
Half-life elimination: Variable: 10 to 100 minutes.
Excretion: Urine (90%); feces (6%).
Effects on bleeding
No information available to require special precautions.
Buy anabolic steroids online USA.
Related products
Superdrol (Methasterone) 20mg tab 100 tabs
$93.00Add to cartMethasterone; Superdrol; Methasteron; UNII-GH88DY98MR; 2alpha,17alpha-Dimethyldihydrotestosterone; NSC 40490.
Dynabol Buy Online in USA 100mg/ml 10 ml Medical Pharma
$93.00Add to cartMetandienone (pINN); Metandienon; Metandienona; Métandiénone; Metandienoni; Metandienonum; Methandrostenolone; NSC-42722. 17β-Hydroxy-17α-methylandrosta-1,4 dien-3-one. Метандиенон.
C20H28O2 = 300.4.
CAS — 72-63-9.
ATC — A14AA03; D11AE01.
ATC Vet — QA14AA03; QD11AE01.
NOTE. The following terms have been used as ‘street names’ or slang names for various forms of Methandienone: Iron Brew.
Pharmacopoeias. In Pol
Equipoise 200mg/ml 10 ml – Medical Pharma
$93.00Add to cartBa-29038; Boldenone Undecylenate (USAN); Boldenone, Undecylenate de; Boldenoni Undecylenas; 1-Dehydrotestosterone (boldenone); Undecilenato de boldenona. 17β-Hydroxyandrosta-1,4-dien-3-one 17-(undec-10-enoate). Болденона Ундециленат.
C30H44O3 = 452.7.
CAS — 846-48-0 (boldenone); 13103-34-9 (boldenone undecenoate).
Equipoise contains: 200mg.
200 mg / ml Boldenone Undecylenate.Pharmacologic Category: Androgen.
Dosing
a) 1 mg/kg IM; may repeat in 1 week intervals (most will respond with one or two treatments).
b) 3 mg/kg IM; repeated at 1 week intervals (Robinson 1987).Provir (Mesterolone) 50mg/tab 100 tabs – Medical Pharma
$93.00Add to cartPharmacologic Category
Androgen.
Dosing: Adult
50mg every days for duration of 4-8 weeks.
Dosing: Geriatric
Refer to adult dosing.
Dosing: Pediatric
No information in pediatric population available.
Dosing: Renal impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution due to propensity to cause edema.
Dosing: Hepatic impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution.