Most Popular steroids USA
-
 Test Enanthate 200mg 20 ml Sydgroup
Original price was: $110.00.$53.00Current price is: $53.00.
Test Enanthate 200mg 20 ml Sydgroup
Original price was: $110.00.$53.00Current price is: $53.00. -
Testosterone Cypionate 300mg 20ml Sydgroup
Original price was: $99.00.$53.00Current price is: $53.00.
-
Somatrox XT Labs 150 IU x 10 vials (15 ui each)
Original price was: $450.00.$350.00Current price is: $350.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00












When testosterone is low, many men notice clear changes: reduced libido, fewer morning erections, creeping fatigue and stubborn abdominal fat. Sexual and reproductive signs often prompt testing, although libido loss can occur without full erectile dysfunction, and fertility deserves a separate discussion because testosterone replacement suppresses sperm production. Mood shifts, trouble concentrating and sleep problems are common as well, and they overlap with depression or obstructive sleep apnea, so symptoms alone do not confirm the diagnosis.
This guide covers how low T typically presents, what to check before a lab draw, and how clinicians confirm deficiency with repeat morning measurements. A short pre-test checklist (improving sleep, avoiding heavy alcohol and reviewing medications) helps reduce false positives and improve accuracy. Later sections explain how providers separate low T from hypothyroidism, anemia or chronic illness and when to discuss treatment and fertility-preserving options with a clinician.
Testosterone Is Low: Key Takeaways You Need to Know
Recognize symptoms: Sexual changes such as low libido and fewer morning erections are the most specific clues, while fatigue, mood shifts and sleep problems also justify testing.
Confirm with labs: A fasting morning total testosterone is the first step; repeat low results and add free testosterone and SHBG when values are borderline or protein binding is suspected.
Reduce false positives: Improve sleep, avoid heavy alcohol and intense exercise before testing, and review medications like opioids, corticosteroids and biotin that can alter results.
Identify causes and risks: Distinguish primary versus secondary hypogonadism and flag red flags such as chemotherapy, testicular injury, prior anabolic steroid use or pituitary symptoms for further workup.
Treatment and monitoring: Start with weight loss and resistance training, then discuss TRT, fertility-preserving strategies and regular lab monitoring with a licensed clinician.
1. Recognize the signs: how low testosterone shows up
Sexual changes are the clearest early signs. Libido loss can occur without full erectile dysfunction, so decreased interest may appear even if erections still happen.
Energy, mood and sleep problems frequently accompany low testosterone but are not specific. Persistent fatigue, low motivation, depressed mood and trouble concentrating are common complaints, and untreated sleep apnea or chronic sleep disruption can cause the same symptoms while lowering testosterone. Laboratory testing is required to separate low T from alternative causes and to guide management decisions.
Physical and metabolic changes provide additional clues. Loss of muscle mass, slower workout recovery, reduced strength and increased central body fat point toward testosterone deficiency, and subtle signs may include gynecomastia or weaker lifts despite consistent training. Track changes over months rather than reacting to a single poor training block, and compare trends with testosterone test results.
- Aim for 7 to 9 hours of sleep on each of the two nights before testing.
- Avoid heavy alcohol for 48 hours and skip intense exercise the morning of the blood draw.
- Schedule a morning fasting blood draw when possible and repeat abnormal results on a separate morning.
- Review prescription and over-the-counter medications with your clinician, calling out opioids, corticosteroids and biotin.
2. How clinicians test: which labs, when and what cutoffs mean
Clinicians start with a total testosterone measurement because it captures most circulating hormone. If the total value is borderline or binding-protein abnormalities are suspected, providers add free or bioavailable testosterone since the free fraction is the biologically active portion. Many laboratories report calculated free testosterone using measured albumin and SHBG to improve consistency across assays. For a plain-language comparison of total versus free testing, see the difference between total and free testosterone tests.
Clinicians commonly use about 300 ng/dL as a practical cutoff. Values below that, together with compatible symptoms, often prompt further evaluation or a discussion of treatment. Reference ranges differ by lab and age, so borderline results in the 230 to 400 ng/dL range are handled case by case and usually require additional measures such as calculated free testosterone, SHBG and pituitary markers like LH and FSH. For age-specific reference considerations, see resources on normal testosterone levels by age.
Common adjunct tests include LH and FSH to localize dysfunction, prolactin to screen for pituitary issues, SHBG and albumin for accurate free testosterone calculation, a CBC to check hematocrit, PSA for prostate screening when age-appropriate, and fasting glucose or HbA1c plus a lipid panel for cardiometabolic risk. These baseline studies create an actionable plan for diagnosis and follow-up.
With test results and clinical context, clinicians identify likely causes and urgent red flags that require referral. The following section reviews common causes and warning signs to watch for.
3. Why testosterone is low: common causes and red flags
Primary hypogonadism is testicular failure from causes such as testicular injury, chemotherapy or genetic conditions like Klinefelter syndrome. Secondary or central hypogonadism comes from the hypothalamus or pituitary, including pituitary tumors or hyperprolactinemia that suppress gonadotropin release. Measuring LH and FSH helps separate the two: high LH and FSH point to primary testicular failure, while low or inappropriately normal levels suggest a secondary cause.
Metabolic and lifestyle factors are common, often reversible contributors. Obesity and type 2 diabetes increase insulin resistance and aromatization of androgens to estrogen in adipose tissue, which lowers circulating testosterone and disrupts feedback loops. Chronic stress, poor sleep or obstructive sleep apnea, excessive alcohol and lack of resistance training also blunt testosterone production, so address weight, sleep and training before irreversible interventions when appropriate. Several clinical reviews summarize metabolic contributors and recovery expectations in men with low testosterone; see a systematic review of testosterone therapy risks and benefits for further reading.
Certain medications and substances suppress the hypothalamic-pituitary-testicular axis. Chronic opioids, some antidepressants and prolonged glucocorticoids are frequent culprits, and prior anabolic steroid cycles can cause prolonged suppression that requires a different management plan. Recovery after steroid use can take months and typically needs specialist input from endocrinology or urology for hormonal support and monitored recovery strategies.
Recognize urgent warning signs that need prompt specialist care. Seek immediate attention for sudden testicular pain, a palpable lump, rapid-onset gynecomastia, new visual changes with headaches that suggest a pituitary mass or markedly abnormal laboratory results. For acute severe symptoms such as intense pain, sudden vision loss or fainting, go to the emergency department without delay.
4. Treatment options: lifestyle first, then medical choices and fertility-safe paths
Begin with targeted lifestyle measures because they are low-risk and often effective. Aim to lose 5 to 10 percent of body weight over 3 to 6 months through calorie-aware nutrition and consistent resistance training three times per week, and many men notice better energy and libido within 8 to 12 weeks. Improve sleep prioritize consistent, adequate sleep before testing, treat obstructive sleep apnea if present, and limit heavy drinking to support hormonal recovery.
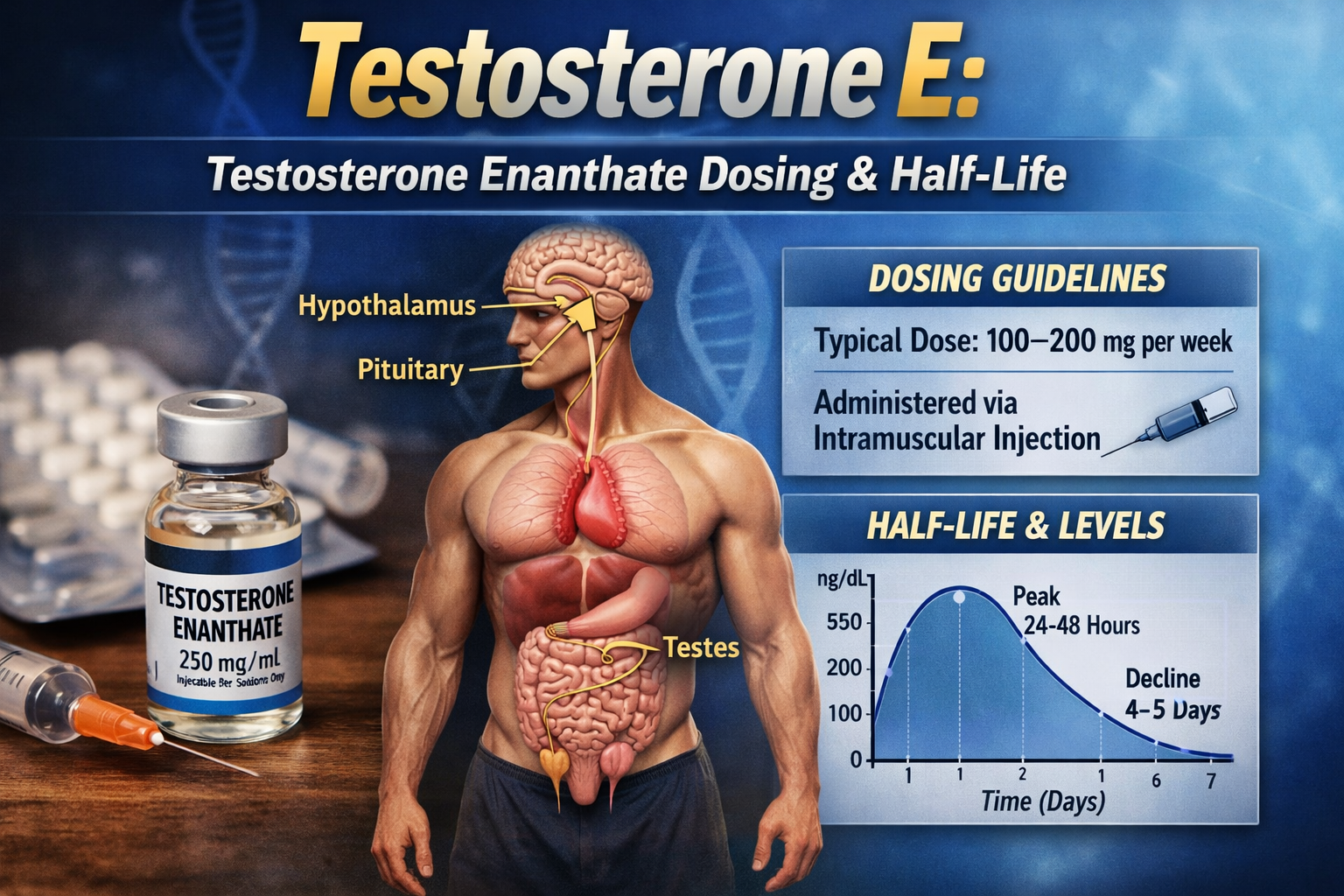
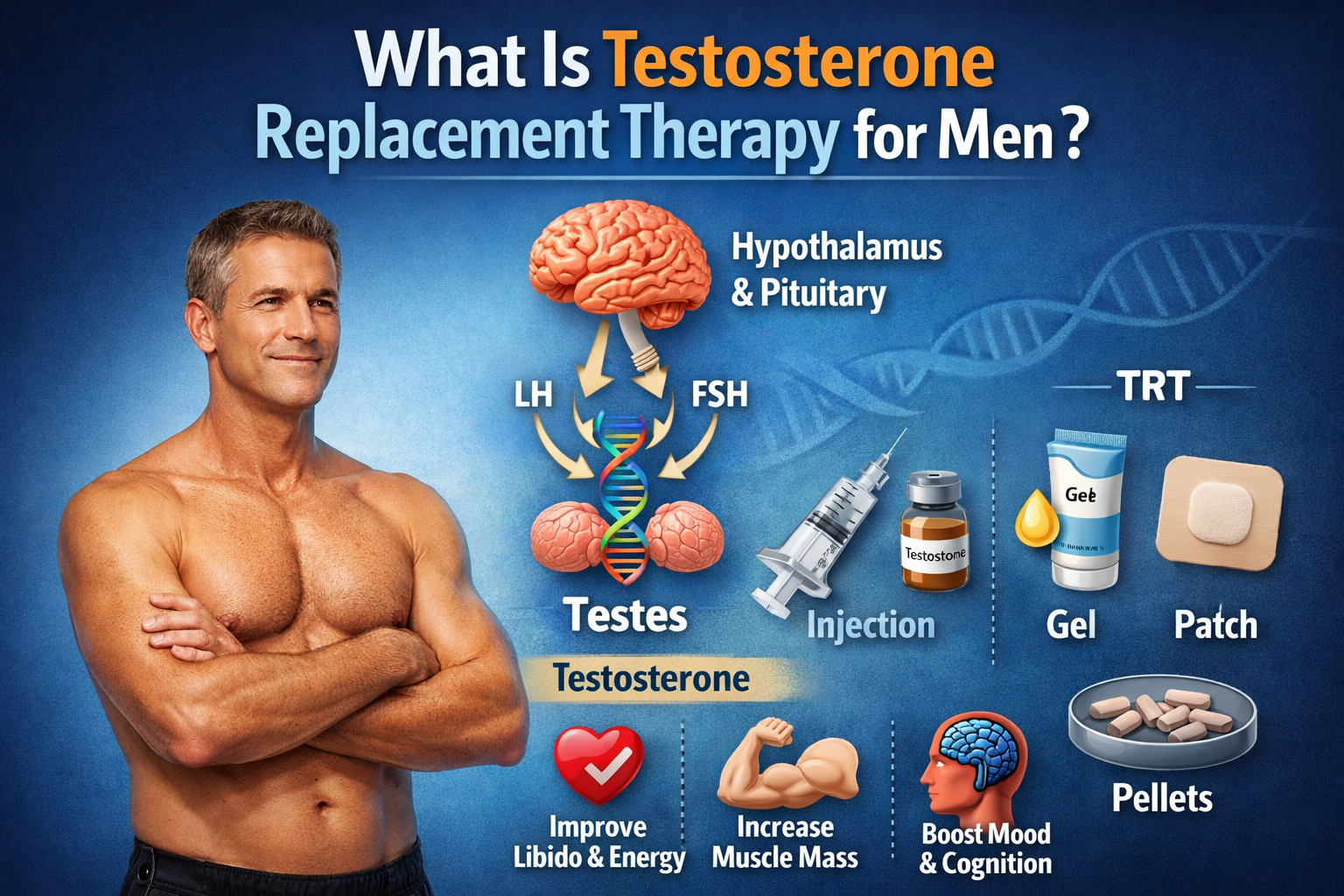
Exogenous testosterone is an option when lifestyle changes are insufficient or symptoms persist despite confirmed low levels. Delivery methods include intramuscular or subcutaneous injections, transdermal gels or patches, and subdermal pellets; expected benefits include improved libido, energy, lean mass and bone density. Risks to discuss include erythrocytosis, potential prostate effects requiring PSA monitoring, suppression of sperm production leading to infertility, possible worsening of sleep apnea and varied cardiovascular study findings.
If fertility matters, consider specialist strategies that preserve spermatogenesis rather than standard exogenous testosterone. Options include clomiphene citrate to stimulate the hypothalamic-pituitary axis, human chorionic gonadotropin to maintain intratesticular testosterone and spermatogenesis, and selective estrogen receptor modulators in selected cases. These approaches require specific monitoring and specialist oversight and are distinct clinical pathways, not weaker versions of replacement therapy.
Plan monitoring proactively. Recheck testosterone 4 to 12 weeks after starting or changing therapy and assess hematocrit every 3 to 6 months initially; obtain a baseline PSA and schedule periodic checks when indicated. Adjust dose or pause therapy for hematocrit elevations above about 52 to 54 percent or for new prostate concerns, and keep clear documentation with regular follow-up visits.
5. Cost-effective TRT without insurance: practical routes and at-home testing
If you need evaluation but lack insurance, several lower-cost routes are available. Telemedicine clinics may offer structured evaluation programs that bundle consultation and laboratory testing at transparent pricing. reducing upfront costs while allowing evaluation and prescriptions when appropriate. Community health centers and walk-in clinics offer affordable in-person assessment, and cash-pay visits with local urologists or endocrinologists can provide better ongoing monitoring when needed.
Shop self-pay lab prices and compare generic medication options to lower testing and treatment expenses. Generic injectable testosterone typically costs less per month than branded gels, and pharmacy discount programs, 90-day supplies and mail-order services can reduce out-of-pocket spending. If a compounded product is considered, verify the pharmacy’s accreditation and quality-control procedures before proceeding.
Validated at-home testing kits can help collect a morning baseline and reduce initial clinic visits, but use only accredited, laboratory-backed kits that provide clear instructions and clinician integration. At-home kits assist with screening and monitoring but do not replace a licensed provider’s diagnosis or prescription. When paying cash, prioritize safety and legality: do not buy prescription testosterone without a valid prescription and avoid unverified suppliers, using licensed pharmacies or telemedicine services that include appropriate monitoring and lab follow-up. If you’re researching online vendors, review reputable resources such as Buy Steroids Online in USA 2025, SteroidsOnlineUSA.com before making decisions.
6. A clear next-step checklist for your clinician visit and monitoring
Before your appointment, prepare a concise symptom diary and a complete list of current medications and supplements, highlighting opioids and biotin by name. Note any past anabolic steroid use with dates, recent weights, sleep patterns and brief details on training and diet so you can provide a clear history. Bring prior lab results to make the visit more productive and often avoid repeat testing.
Request a focused starter lab panel and bring copies to the visit: a morning total testosterone, plus free testosterone or SHBG if values are borderline, as well as LH and FSH and prolactin. Include a CBC with hematocrit, PSA if age-appropriate, and fasting glucose or HbA1c with a lipid panel to assess cardiometabolic risk. For plain-language information about what a testosterone blood test measures and how to prepare, see the test overview at MedlinePlus. Ask your clinician how often they will repeat labs based on the chosen therapy and baseline risks.
Ask direct questions such as “Is this likely primary or secondary hypogonadism?”, “What are my treatment options and the fertility implications?” and “What monitoring schedule will you use and what are the criteria for stopping or adjusting therapy?” Use shared decision-making and prioritize nonpharmacologic measures when possible, and do not self-administer testosterone: work with a licensed provider for prescriptions, monitoring and follow-up.
Frequently Asked Questions About Low Testosterone
Why my testosterone is low?
Testosterone can be low for many reasons. Common causes include obesity, poor sleep, chronic stress, excessive alcohol use, type 2 diabetes, and certain medications such as opioids or corticosteroids.
Medical causes may involve the testicles (primary hypogonadism) or the pituitary gland (secondary hypogonadism). Blood tests measuring testosterone along with LH and FSH help determine the underlying cause.
What happens when testosterone is low?
When testosterone is low, many men notice reduced libido, fewer morning erections, fatigue, increased abdominal fat, and decreased muscle mass. Mood changes, lower motivation, and difficulty concentrating can also occur.
If deficiency is persistent and untreated, it may contribute to reduced bone density and metabolic changes over time.
Why testosterone is low?
Testosterone levels may decline due to aging, metabolic conditions, sleep disorders such as obstructive sleep apnea, medication effects, or hormonal signaling problems in the brain.
Sometimes the cause is reversible, especially when related to weight, stress, or lifestyle factors. Proper testing is required to identify the specific reason.
What is low testosterone in women?
Women produce testosterone in smaller amounts than men. In women, low testosterone may be associated with decreased libido, fatigue, and reduced sense of well-being, particularly after menopause.
Diagnosis and treatment thresholds differ significantly from men, and management should be guided by a clinician experienced in female hormone health.
How to know testosterone if is low?
The only reliable way to know if testosterone is low is through a blood test. Doctors typically measure total testosterone in the morning when levels are highest.
If results are borderline, free testosterone and SHBG may be evaluated. Symptoms alone are not enough to confirm the diagnosis.
How to tell testosterone is low?
Possible signs include low sex drive, fewer morning erections, persistent fatigue, reduced strength, and increased body fat. However, these symptoms overlap with other conditions such as depression or sleep disorders.
Because of this overlap, laboratory testing is necessary to confirm whether testosterone is truly low.
How is low testosterone diagnosis?
Low testosterone is diagnosed through a combination of symptoms and repeat morning blood tests. Most clinical guidelines use approximately 300 ng/dL as a practical reference point, interpreted alongside symptoms.
Additional tests such as LH, FSH, and prolactin may help determine whether the issue originates in the testicles or the pituitary gland.
Why is low testosterone bad?
Low testosterone is not immediately dangerous in every case, but persistent deficiency can affect quality of life. It may contribute to reduced muscle mass, increased visceral fat, lower bone density, mood changes, and fertility suppression.
The impact depends on severity, duration, and underlying cause.
Is low testosterone good?
In adult men, clinically low testosterone is generally not considered beneficial. However, temporary decreases can occur during illness, caloric restriction, or periods of high stress and may normalize afterward.
Treatment is typically only considered when low levels are persistent, confirmed by testing, and associated with symptoms.
How can I increase low testosterone levels naturally?
Natural strategies focus on improving hormonal signaling rather than directly replacing testosterone. The most evidence-supported approaches include:
- Losing excess body fat (even 5–10% weight loss can improve levels)
- Resistance training 3–4 times per week
- Sleeping 7–9 hours consistently
- Treating obstructive sleep apnea if present
- Reducing heavy alcohol intake
- Managing chronic stress and overtraining
- Ensuring adequate dietary protein and healthy fats
If testosterone remains low despite lifestyle optimization, medical evaluation is recommended.
What are common signs of low testosterone in men?
Common signs include:
- Reduced libido
- Fewer morning erections
- Fatigue and low energy
- Decreased muscle mass and strength
- Increased abdominal fat
- Depressed mood or irritability
- Difficulty concentrating
Because these symptoms overlap with other conditions, blood testing is necessary for confirmation.
What are the best supplements for low testosterone available online?
Most over-the-counter “testosterone boosters” do not significantly increase testosterone in men with clinically low levels. Some ingredients such as vitamin D, zinc, magnesium, and ashwagandha may support normal hormonal function in individuals who are deficient, but they do not replace medical therapy for confirmed hypogonadism.
Consumers should be cautious of exaggerated claims. Supplements are not regulated like prescription medications, and quality can vary. If testosterone deficiency is confirmed, prescription treatment under medical supervision is more reliable than online supplements.
How is low testosterone officially diagnosed by medical professionals?
Low testosterone is diagnosed through both symptoms and laboratory confirmation. Physicians typically:
- Measure total testosterone in the early morning (fasting when possible).
- Repeat the test on a separate morning to confirm.
- Evaluate free testosterone if results are borderline.
- Order additional labs (LH, FSH, prolactin) to determine whether the cause is primary or secondary.
Diagnosis is not based on symptoms alone.
Which clinics specialize in testosterone replacement therapy near me?
Clinics that manage testosterone replacement therapy (TRT) are typically:
- Endocrinology practices
- Urology clinics
- Men’s health clinics
- Some primary care physicians with hormone management experience
To find reputable providers, search for board-certified endocrinologists or urologists in your area. Telemedicine clinics also offer hormone evaluation in many regions, but ensure they provide proper lab monitoring and follow established clinical guidelines.
Overview of available treatments for low testosterone levels.
Treatment options depend on severity, symptoms, and fertility goals.
Lifestyle optimization is the first step. If levels remain low and symptomatic, medical options include:
- Injectable testosterone (intramuscular or subcutaneous)
- Transdermal gels or patches
- Subdermal pellets
For men who wish to preserve fertility, alternatives such as clomiphene citrate or hCG may be considered to stimulate natural production rather than replace testosterone directly.
All treatments require medical monitoring.
Are there any reliable at-home testosterone test kits I can order?
Some laboratory-backed at-home kits allow you to collect a finger-prick or saliva sample and send it to a certified lab. Reliable kits should:
- Use CLIA-certified laboratories
- Provide clear instructions
- Offer clinician-reviewed results
At-home tests can be useful for screening but do not replace formal medical diagnosis, especially since repeat morning testing is often required.
Find specialized clinics for male hormone therapy near me.
Specialized hormone therapy clinics are usually found under:
- Endocrinology centers
- Urology groups
- Men’s health or andrology clinics
When choosing a clinic, look for licensed medical providers, structured lab monitoring, transparent pricing, and adherence to Endocrine Society or AUA guidelines.
Avoid providers that prescribe testosterone without proper testing.
What prescription options exist for treating low testosterone?
Prescription options include:
- Testosterone cypionate or enanthate injections
- Testosterone gels
- Testosterone patches
- Testosterone pellets
Alternative prescriptions (when fertility preservation is important) may include:
- Clomiphene citrate
- Human chorionic gonadotropin (hCG)
Each option has different dosing schedules, costs, and monitoring requirements.
Cost analysis of different testosterone replacement therapies.
Costs vary by formulation and region:
- Injectable testosterone is typically the most affordable option.
- Gels and patches are usually more expensive.
- Pellets often have higher upfront procedural costs.
- Telemedicine programs may bundle labs and consultations.
Additional costs may include laboratory monitoring (testosterone levels, hematocrit, PSA) every 3–6 months.
Insurance coverage varies widely, and generic injectable testosterone is generally the most cost-effective long-term option.
References (APA 7th Edition)
American Urological Association. (2018). Evaluation and management of testosterone deficiency: AUA guideline. The Journal of Urology, 200(2), 423–432. https://doi.org/10.1016/j.juro.2018.03.115
Bhasin, S., Brito, J. P., Cunningham, G. R., Hayes, F. J., Hodis, H. N., Matsumoto, A. M., Snyder, P. J., Swerdloff, R. S., Wu, F. C. W., & Yialamas, M. A. (2018). Testosterone therapy in men with hypogonadism: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 103(5), 1715–1744. https://doi.org/10.1210/jc.2018-00229
Bhasin, S., Cunningham, G. R., Hayes, F. J., Matsumoto, A. M., Snyder, P. J., Swerdloff, R. S., & Montori, V. M. (2010). Testosterone therapy in men with androgen deficiency syndromes: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 95(6), 2536–2559. https://doi.org/10.1210/jc.2009-2354
Corona, G., Goulis, D. G., Huhtaniemi, I., Zitzmann, M., Toppari, J., Forti, G., & Maggi, M. (2020). The effect of testosterone supplementation on depression and sexual function in men: A meta-analysis. The Journal of Clinical Endocrinology & Metabolism, 105(3), 1–14. https://doi.org/10.1210/clinem/dgz257
Corona, G., Vignozzi, L., Sforza, A., Maggi, M., & Mannucci, E. (2016). Obesity and late-onset hypogonadism. Molecular and Cellular Endocrinology, 418(Pt 2), 120–133. https://doi.org/10.1016/j.mce.2015.10.012
Grossmann, M. (2011). Low testosterone in men with type 2 diabetes: Significance and treatment. The Journal of Clinical Endocrinology & Metabolism, 96(8), 2341–2353. https://doi.org/10.1210/jc.2011-0118
Mulhall, J. P., Trost, L. W., Brannigan, R. E., Kurtz, E. G., Redmon, J. B., Chiles, K. A., Lightner, D. J., Miner, M. M., Murad, M. H., Nelson, C. J., Platz, E. A., Ramanathan, L. V., Lewis, R. W., & Parish, S. J. (2018). Evaluation and management of testosterone deficiency: AUA guideline. The Journal of Urology, 200(2), 423–432. https://doi.org/10.1016/j.juro.2018.03.115
Qu, H., Zhang, Y., Li, Y., Li, S., & Wang, Y. (2022). Obstructive sleep apnea and serum total testosterone: A systematic review and meta-analysis. Sleep and Breathing, 26, 1–10. https://doi.org/10.1007/s11325-022-02655-6
Snyder, P. J., Peachey, H., Berlin, J. A., Hannoush, P., Haddad, G., Dlewati, A., Santanna, J., Loh, L., Lenrow, D. A., Holmes, J. H., Kapoor, S. C., Atkinson, L. E., & Strom, B. L. (2000). Effects of testosterone replacement in hypogonadal men. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2670–2677. https://doi.org/10.1210/jcem.85.8.6731
Trost, L. W., & Mulhall, J. P. (2016). Challenges in testosterone measurement and interpretation. The Journal of Sexual Medicine, 13(6), 1027–1036. https://doi.org/10.1016/j.jsxm.2016.03.371
Turek, P. J., Williams, R. H., Gilbaugh, J. H., & Lipshultz, L. I. (1995). The reversibility of anabolic steroid-induced azoospermia. The Journal of Urology, 153(5), 1628–1630. https://doi.org/10.1016/S0022-5347(01)67347-0
Author Bio
Dr. Michael R. Halvorsen, MD, FACE
Dr. Michael R. Halvorsen is a board-certified endocrinologist specializing in male reproductive endocrinology, testosterone deficiency, and metabolic hormone disorders. He completed his medical degree at the University of Michigan Medical School and his fellowship in Endocrinology, Diabetes, and Metabolism at Johns Hopkins University.
With over 15 years of clinical experience, Dr. Halvorsen focuses on evidence-based evaluation and management of hypogonadism, fertility-preserving hormone therapies, obesity-related testosterone suppression, and pituitary disorders. He has treated thousands of patients with both primary and secondary hypogonadism and regularly collaborates with urologists and reproductive specialists on complex hormonal cases.
Dr. Halvorsen has authored peer-reviewed publications on androgen physiology, metabolic syndrome, and testosterone therapy safety monitoring. He is a Fellow of the American College of Endocrinology (FACE) and a member of the Endocrine Society and the American Association of Clinical Endocrinology.
His clinical approach emphasizes:
- Proper diagnostic confirmation with repeat morning testing
- Differentiating primary vs. secondary hypogonadism
- Fertility-preserving strategies when indicated
- Cardiometabolic risk assessment before therapy
- Careful hematologic and prostate monitoring during treatment
Dr. Halvorsen advocates for lifestyle-first interventions when appropriate and follows current Endocrine Society and AUA guidelines when prescribing testosterone therapy.