Most Popular steroids USA
-
 Trenbolone 200 20ml - Sydgroup
$53.00
Trenbolone 200 20ml - Sydgroup
$53.00 -
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.












Testosterone Propionate 100mg 10ml – Bangkok Pharmaceuticals
$93.00
Testosterone Propionate is a commonly manufactured injectable form of the primary male androgen Testosterone. The added Propionate ester will slow the rate in which Testosterone is released from the injection site, but only for a few days.
Testosterone Propionate is, therefore, comparatively much faster acting than other Testosterone esters such as Cypionate or Enanthate, and requires a much more frequent dosing schedule.
By most accounts Testosterone Propionate is an older and cruder form of injectable Testosterone, made obsolete by the slower acting and more comfortable esters that were developed subsequent to it. Still, those who are not bothered by the frequent injection schedule find Testosterone Propionate every bit as acceptable.
As an injectable Testosterone, it is a powerful mass building drug, capable of producing rapid gains in both muscle size and strength.
Testosterone Propionate 100mg 10ml – Bangkok Pharmaceuticals Steroids USA
History
:
Testosterone Propionate was first described in 1935, during a series of experiments that set out to increase the therapeutic usefulness of Testosterone by slowing its release into the bloodstream. Two years later, Schering AG in Germany would introduce the first Testosterone Propionate product under the brand name Testoviron®. Propionate was also the first commercially available injectable ester of Testosterone on the U.S. prescription drug market, and remained the dominant form of Testosterone globally before 1960.
Back during the early 1950’s, for example, when steroids were first being experimented with by small numbers of American athletes, the only readily available anabolic/androgenic steroids were Methyltestosterone, Testosterone Propionate, and Testosterone suspension. Interesting enough, during this time Testosterone Propionate was also available in orally administered (Buccal) preparations, but they disappeared from the U.S. market during the 1980’s.
Early prescribing guidelines for Testosterone Propionate called for a number of therapeutic uses. It was mainly applied to cases of male androgen insufficiency, and those issues normally surrounding low Testosterone levels such as reduced sex drive and impotence in adults, and cryptorchidism (undescended testicles) in teenagers and young adults.
But it also had such other uses as treating menopause, menorrhagia (heavy menstrual bleeding), menstrual tension, chronic cystic mastitis (fibrocystic breasts), endometriosis, and excessive lactation, covering a wide range of situations in which the male hormone Testosterone was being applied to female patients. Over the years these wide guidelines were narrowed by the U.S. Food & Drug Administration, however, and by the 1980’s, Testosterone Propionate was being largely applied only to male patients.
Testosterone Propionate has a long history of availability in the U.S. and abroad, and remains a very common form of Testosterone on the global market to this day. It must be emphasized, however, that its ability to remain on the market is more a product of history than unique application. Testosterone Propionate was the first acceptable ester of Testosterone, and consequently has many decades of history as a useable therapeutic agent.
Many companies have sold it for decades now, and so long as it is still in demand will continue to do so. But other (more modern) forms of Testosterone such as Enanthate and Cypionate are much more popular today, as they are much slower acting still, and allow for far more comfortable administration schedules. Testosterone Propionate is still approved for sale in the United States, although its ultimate market future here remains questionable.
Bodybuilders commonly consider propionate to be the mildest Testosterone ester, and the preferred form of this hormone for dieting/cutting phases of training. Some will go so far as to say that Propionate will harden the physique, while giving the user less water and fat retention than one typically expects to see with a Testosterone like Enanthate, Cypionate or Sustanon. Realistically, however, these advantages do not hold up to close scrutiny.
The Propionate ester is actually removed before the Testosterone it carries is active in the body, and ultimately has little effect outside of slowing steroid release. It all really boils down to how much Testosterone you are getting into your blood with each particular esterified compound. Otherwise, there are no real functional differences between them.
How Supplied:
Testosterone Propionate is widely available in human and veterinary drug markets. Composition and dosage may vary by country and manufacturer, but usually contain 25 mg/ml, 50 mg/ml, or 100 mg/ml of steroid dissolved in oil.
Structural Characteristics:
Testosterone Propionate is a modified form of Testosterone, where a carboxylic acid ester (propionic acid) has been attached to the 17-beta hydroxyl group. Esterified forms of testosterone are less polar than free Testosterone, and are absorbed more slowly from the area of injection. Once in the bloodstream, the ester is removed to yield free (active) Testosterone.
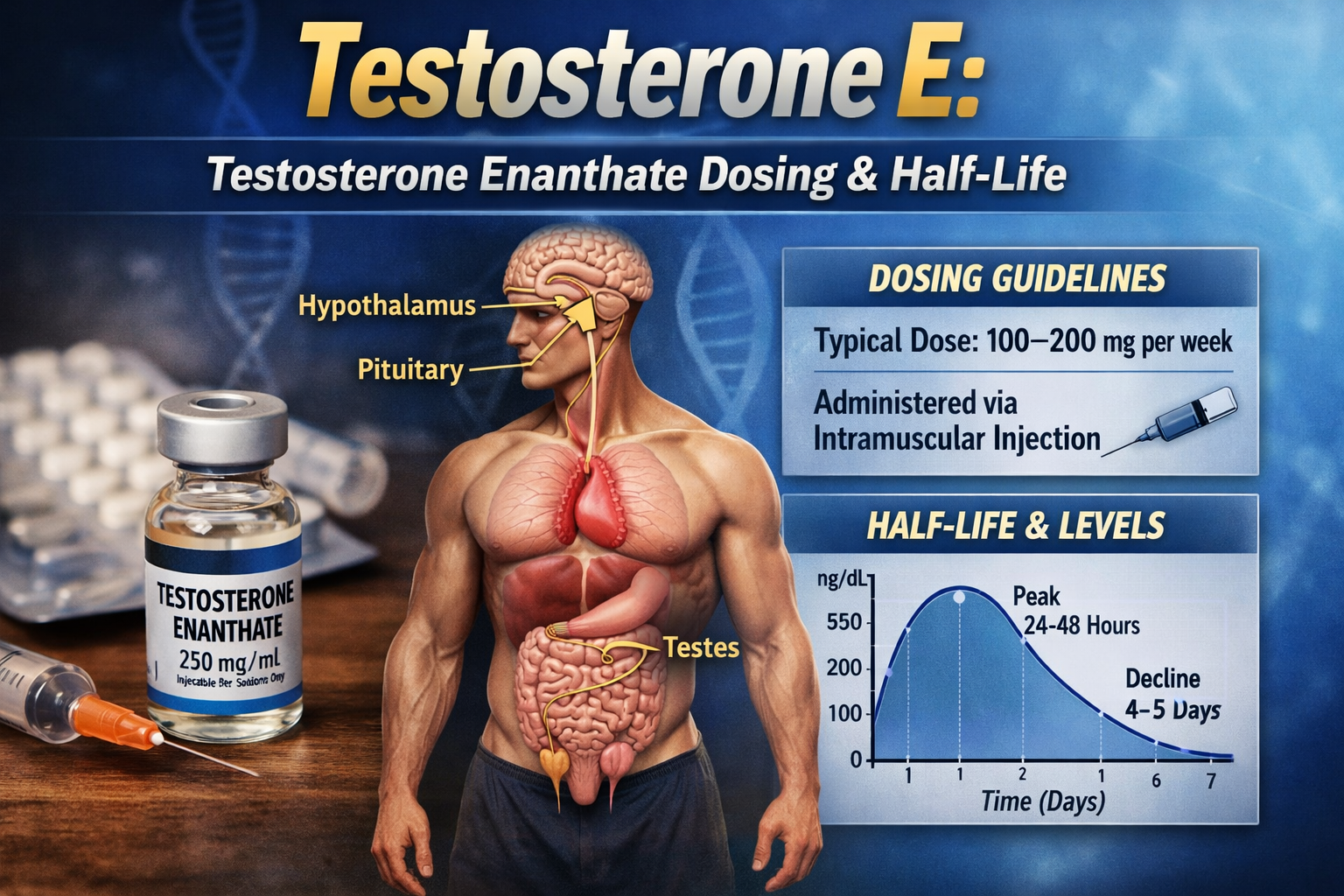
Esterified forms of Testosterone are designed to prolong the window of therapeutic effect following administration, allowing for a less frequent injection schedule compared to injections of free (unesterified) steroid. The half-life of Testosterone Propionate is approximately two days after injection.
Figure 1. Pharmacokinetics of 25 mg labeled Testosterone Propionate injection. Source: Pharmacokinetic properties of Testosterone Propionate in normal men. Fujioka M, Shinohara Y,Baba S. et.Al. J Clin Endocrinol Metab 63 (1986):1361- 4.
Side effects (estrogenic):
Testosterone is readily aromatized in the body to estradiol (estrogen). The aromatase (estrogen synthetase) enzyme is responsible for this metabolism of Testosterone. Elevated estrogen levels can cause side effects such as increased water retention, body fat gain, and Gynecomastia. Testosterone is considered a moderately estrogenic steroid.
An anti-estrogen such as Clomiphene Citrate or tamoxifen citrate may be necessary to prevent estrogenic side effects. One may alternately use an aromatase inhibitor like Arimidex® (Anastrozole), which more efficiently controls estrogen by preventing its synthesis. Aromatase inhibitors can be quite expensive in comparison to anti-estrogens, however, and may also have negative effects on blood lipids.
Estrogenic side effects will occur in a dose dependant manner, with higher doses (above normal therapeutic levels) of Testosterone Propionate more likely to require the concurrent use of an anti-estrogen or aromatase inhibitor. Since water retention and loss of muscle definition are common with higher doses of Testosterone, this drug is usually considered a poor choice for dieting or cutting phases of training. Its moderate estrogenicity makes it more ideal for bulking phases, where the added water retention will support raw strength and muscle size, and help foster a stronger anabolic environment.
Side effects (androgenic):
Testosterone is the primary male androgen, responsible for maintaining secondary male sexual characteristics. Elevated levels of Testosterone are likely to produce androgenic side effects including oily skin, acne, and body/facial hair growth. Men with a genetic predisposition for hair loss (androgenetic alopecia) may notice accelerated male pattern balding. Those concerned about hair loss may find a more comfortable option in nandrolone decanoate, which is a comparably less androgenic steroid.
Women are warned of the potential virilizing effects of anabolic/androgenic steroids, especially with a strong androgen such as Testosterone. These may include deepening of the voice, menstrual irregularities, changes in skin texture, facial hair growth, and clitoral enlargement.
In androgen-responsive target tissues such as the skin, scalp, and prostate, the high relative androgenicity of Testosterone is dependant on its reduction to Dihydrotestosterone (DHT). The 5-alpha reductase enzyme is responsible for this metabolism of Testosterone. The concurrent use of a 5-alpha reductase inhibitor such as finasteride or dutasteride will interfere with site specific potentiation of Testosterone action, lowering the tendency of testosterone drugs to produce androgenic side effects.
It is important to remember that both anabolic and androgenic effects are mediated via the cytosolic androgen receptor. Complete separation of Testosterone’s anabolic and androgenic properties is not possible, even with total 5-alpha reductase inhibition.
Side effects (hepatotoxicity):
Testosterone does not have hepatotoxic effects; liver toxicity is unlikely. One study examined the potential for hepatotoxicity with high doses of Testosterone by administering 400 mg of the hormone per day (2,800 mg per week) to a group of male subjects.
The steroid was taken orally so that higher peak concentrations would be reached in hepatic tissues compared to intramuscular injections. The hormone was given daily for 20 days, and produced no significant changes in liver enzyme values including serum albumin, bilirubin, alanine-amino-transferase, and alkaline phosphatases.
Side effects (cardiovascular):
Anabolic/androgenic steroids can have deleterious effects on serum cholesterol. This includes a tendency to reduce HDL (good) cholesterol values and increase LDL (bad) cholesterol values, which may shift the HDL to LDL balance in a direction that favors greater risk of arteriosclerosis. The relative impact of an anabolic/androgenic steroid on serum lipids is dependant on the dose, route of administration (oral vs. injectable), type of steroid (aromatizable or non-aromatizable), and level of resistance to hepatic metabolism.
Anabolic/androgenic steroids may also adversely affect blood pressure and triglycerides, reduce endothelial relaxation, and support left ventricular hypertrophy, all potentially increasing the risk of cardiovascular disease and myocardial infarction.
Testosterone tends to have a much less dramatic impact on cardiovascular risk factors than synthetic steroids. This is due in part to its openness to metabolism by the liver, which allows it to have less effect on the hepatic management of cholesterol. The aromatization of Testosterone to estradiol also helps to mitigate the negative effects of androgens on serum lipids.
In one study, 280 mg per week of Testosterone ester (Enanthate) had a slight but not statistically significant effect on HDL cholesterol after 12 weeks, but when taken with an aromatase inhibitor a strong (25%) decrease was seen.568 Studies using 300 mg of Testosterone ester (Enanthate) per week for twenty weeks without an aromatase inhibitor demonstrated only a 13% decrease in HDL cholesterol, while at 600 mg the reduction reached 21%. The negative impact of aromatase inhibition should be taken into consideration before such drug is added to Testosterone therapy.
Due to the positive influence of estrogen on serum lipids, Tamoxifen Citrate or Clomiphene Citrate are preferred to aromatase inhibitors for those concerned with cardiovascular health, as they offer a partial estrogenic effect in the liver. This allows them to potentially improve lipid profiles and offset some of the negative effects of androgens. With doses of 600 mg or less of Testosterone per week, the impact on lipid profile tends to be noticeable but not dramatic, making an anti-estrogen (for cardioprotective purposes) perhaps unnecessary.
Doses of 600 mg or less per week have also failed to produce statistically significant changes in LDL/VLDL cholesterol, triglycerides, apolipoprotein B/C-III, C-reactive protein, and insulin sensitivity, all indicating a relatively weak impact on cardiovascular risk factors.570 When used in moderate doses, injectable testosterone esters are usually considered to be the safest of all anabolic/androgenic steroids.
To help reduce cardiovascular strain it is advised to maintain an active cardiovascular exercise program and minimize the intake of saturated fats, cholesterol, and simple carbohydrates at all times during active AAS administration. Supplementing with fish oils (4 grams per day) and a natural cholesterol/antioxidant formula such as Lipid Stabil or a product with comparable ingredients is also recommended.
Side effects (Testosterone suppression):
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous Testosterone production. Testosterone is the primary male androgen, and offers strong negative feedback on endogenous Testosterone production. Testosterone based drugs will, likewise, have a strong effect on the hypothalamic regulation of natural steroid hormones.
Without the intervention of Testosterone stimulating substances, Testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.
The above side effects are not inclusive. For more detailed discussion of potential side effects.
Administration (general):
Testosterone Propionate is often regarded as a painful injection. This is due to the very short carbon chain of the propionic acid ester, which can be irritating to tissues at the site of injection. Many sensitive individuals choose to stay away from this steroid completely, their bodies reacting with a pronounced soreness and low grade fever that may last for a few days after each injection.
Even the mild soreness that is experienced by most users can be quite uncomfortable, especially when you take into account that the drug is being administered multiple times each week for a number of consecutive weeks.
Administration (men):
To treat androgen insufficiency, early prescribing guidelines recommended a dosage of 25 mg given two to three times per week.
Modern product literature usually recommends 25 mg to 50 mg given two to three times per week for the same purpose. The usual dosage among male athletes is in the range of 50-100 mg per injection, which is given every second or third day. Similar to other esters of Testosterone, Testosterone Propionate is commonly used at a weekly cumulative dosage between 200 mg to 400 mg. This level is sufficient for most users to notice exceptional gains in muscle size and strength.
Testosterone Propionate is usually incorporated into bulking phases of training, when added water retention will be of little consequence, the user more concerned with raw mass than definition. Some do incorporate this drug into cutting cycles as well, but typically in lower doses (100-200 mg per week) and/or when accompanied by an aromatase inhibitor to keep estrogen levels under control.
Testosterone Propionate is a very effective anabolic drug, and is often used alone with great benefit. Some, however, find a need to stack it with other anabolic/androgenic steroids for a stronger effect, in which case an additional 200-400 mg per week of Boldenone Undecylenate, Methenolone Enanthate, or Nandrolone Decanoate should provide substantial results with no significant hepatotoxicity. Testosterone is ultimately very versatile, and can be combined with many other anabolic/androgenic steroids to tailor the desired effect.
Administration (women):
Testosterone Propionate is rarely used with women in clinical medicine. When applied, it is most often used as a secondary medication during inoperable breast cancer, when other therapies have failed to produce a desirable effect and suppression of ovarian function is necessary. Testosterone Propionate is not recommended for women for performance enhancing purposes due to its strong androgenic nature and tendency to produce virilizing side effects.
Female bodybuilders who insist on using Testosterone, however, often choose propionate, as blood levels are easier to control with this ester compared to cypionate or enanthate. Should virilization symptoms develop, hormone levels will decline in a matter of days, instead of weeks, following drug cessation. The administration schedule is often more conservative as well, with a small injection (25 mg at most) given every 5 to 7 days, and cycle duration limited to 6-8 weeks or less.
Availability:
Testosterone Propionate is subject to decreasing supply as a pharmaceutical product. Longer acting esters such as Cypionate and Enanthate are much better suited for virtually every clinical application. As such, most physicians and pharmaceutical companies have abandoned this old ester of Testosterone. With a few exceptions in the west, the remaining legitimate supply largely comes from manufacturers in loosely regulated markets of Asia, where black market demand continues to drive production.
References:
566. Miescher, Wettstein & Tschopp (1936) Schweiz. Med. Wschr. 66, 310.
567. Enzyme induction by oral testosterone. Johnsen SG, Kampmann JP, Bennet EP, Jorgensen F 1976 Clin Pharmacol Ther 20:233-237.
568. High-density lipoprotein cholesterol is not decreased if an aromatizable androgen is administered. Friedl K, Hannan C et al. Metabolism 39(1) 1990:
69-74.
569. Testosterone dose-response relationships in healthy young men. Bhasin S, Woodhouse L et al. Am J Physiol Endocrinol Metab 281: E1172-81, 2001.
570. The effects of varying doses of T on insulin sensitivity, plasma lipids, apolipoproteins, and C-reactive protein in healthy young men. Atam Singh, Stanley Hsia, et al. J Clin Endocrinol Metab 87: 136-43, 2002
Related products
Decadurabolin “Decabol” 300mg/ml 10 ml – Medical Pharma
$93.00Add to cartDecanoato de nandrolona; Nandrolon-dekanoát; Nandrolone, décanoate de; Nandroloni decanoas; Nandrolonu dekanonian; Nortestosterone Decanoate; Nortestosterone Decylate. 3-Oxoestr-4-en-17β-yl decanoate; 17β-Hydroxyestr-4-en-3-one decanoate. Нандролона Деканоат.
C28H44O3 = 428.6.
CAS — 360-70-3.
ATC — A14AB01; S01XA11.
ATC Vet — QA14AB01; QS01XA11.Pharmacopoeias. In Eur.(see p.vii) and US.
Espirol (Clenbuterol ) 25mcg 100 tabs – Medical Pharma
$69.00Add to cartClenbutérol, chlorhydrate de; Clenbuteroli hydrochloridum; Hidrocloruro de clenbuterol; Klenbuterol hydrochlorid; Klenbuterolhidroklorid; Klenbuterolhydroklorid; Klenbuterolihydrokloridi; Klenbuterolio hidrochloridas; NAB-365 (clenbuterol). 1-(4-Amino-3,5-dichlorophenyl)-2-tert-butylaminoethanol hydrochloride.
Testosterone Online Purchase Enanthate 250mg/ml MP
$93.00Add to cartC26H40O3 = 400.6.
CAS — 315-37-7.
ATC — G03BA03.
ATC Vet — QG03BA03.USP 31(Testosterone Enanthate). A white or creamy-white crystalline powder. It is odourless or has a faint odour characteristic of heptanoic acid. Insoluble in water; very soluble in ether; soluble in vegetable oils. Store at a temperature of 2°to 8°. Protect from light.
Testosterone E contains: 250mg 250 mg / ml Testosterone Enanthate.
Mastabol 100mg/ml 10ml – Medical Pharma Buy in USA
$93.00Add to cartMastabol 100mg/ml (10ml) by Medical Pharma is a premium Drostanolone Propionate formula designed to enhance muscle hardness, strength, and fat loss. Ideal for cutting cycles, it promotes a lean, defined physique while maintaining high performance. Available for secure purchase in the USA with fast shipping and a trusted buying process.