Most Popular steroids USA
-
 Test Enanthate 200mg 20 ml Sydgroup
Original price was: $110.00.$53.00Current price is: $53.00.
Test Enanthate 200mg 20 ml Sydgroup
Original price was: $110.00.$53.00Current price is: $53.00. -
Testosterone Cypionate 300mg 20ml Sydgroup
Original price was: $99.00.$53.00Current price is: $53.00.
-
Somatrox XT Labs 150 IU x 10 vials (15 ui each)
Original price was: $450.00.$350.00Current price is: $350.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00












Test Enanthate 200mg 20 ml Sydgroup
Original price was: $110.00.$53.00Current price is: $53.00.
Test Enanthate 200mg 20ml Sydgroup
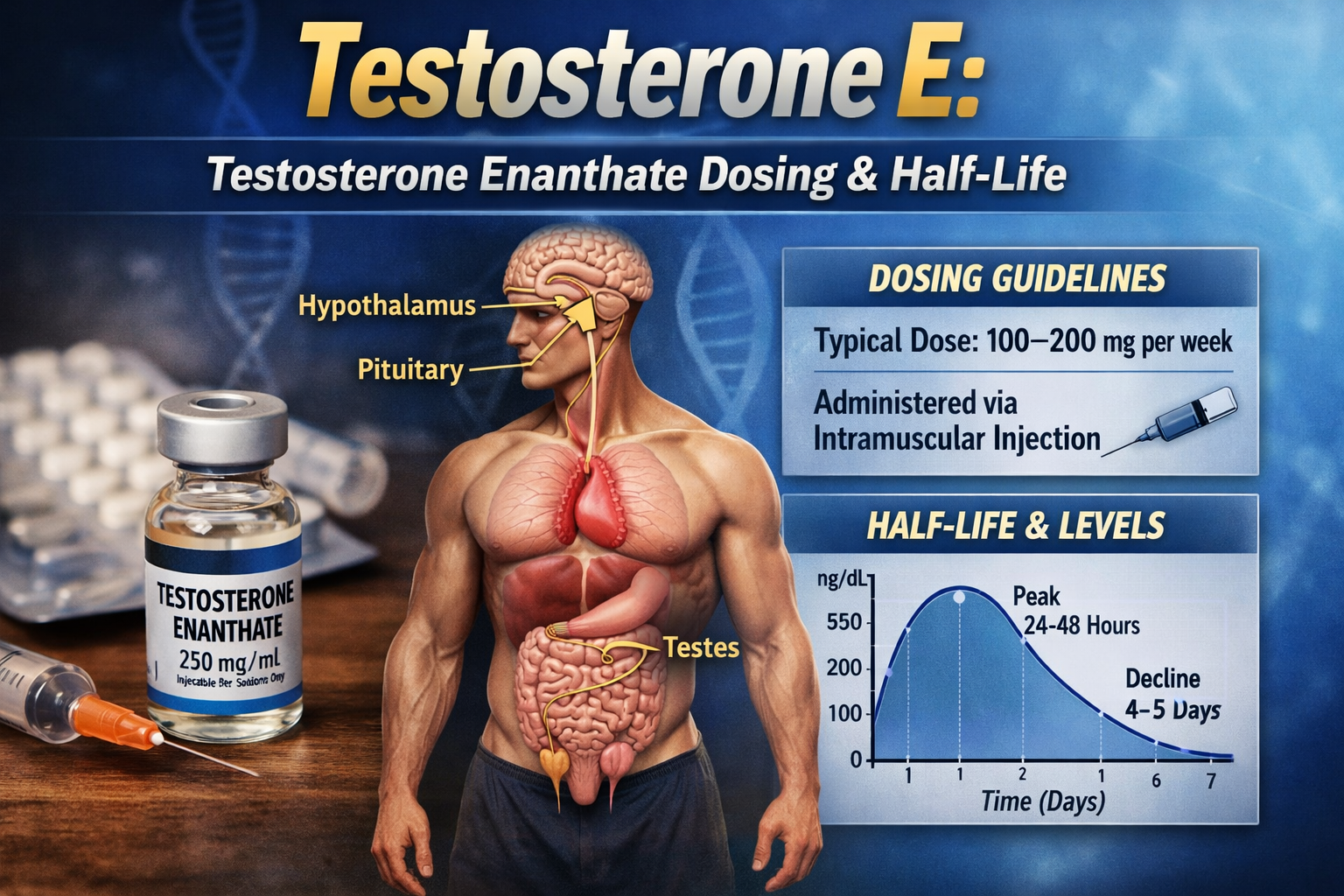
Test Enanthate 200mg 20ml by Sydgroup is a long-acting injectable testosterone enanthate formulation designed to provide sustained testosterone release after intramuscular administration. In the context of testosterone replacement therapy and performance-related discussions, its 200mg/ml concentration allows for structured dosing while maintaining the pharmacokinetic advantages of the enanthate ester, including gradual absorption, stable serum testosterone support, and reduced injection frequency compared with short-acting testosterone preparations.
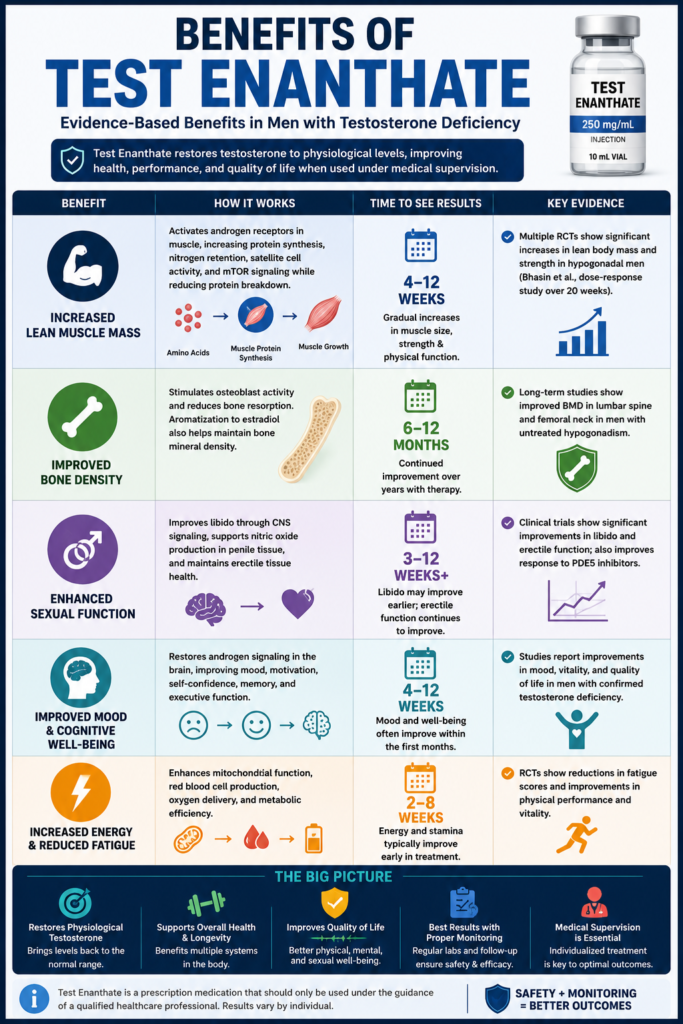
Unlocking Test Enanthate: Benefits, Uses, and Best Practices
Unlock the potential of Test Enanthate! Discover its myriad benefits, uses, and best practices to enhance your fitness journey and promote optimal growth.
What Is Test Enanthate?
Testosterone Enanthate is a long-acting injectable testosterone ester widely used in modern medicine to treat male hypogonadism, a condition in which the body does not produce adequate amounts of testosterone. By attaching the naturally occurring testosterone molecule to an enanthate ester (heptanoate chain), scientists created a formulation that is released gradually after intramuscular injection, allowing for more stable serum testosterone concentrations compared with unesterified testosterone.
Unlike oral testosterone formulations, Testosterone Enanthate bypasses first-pass hepatic metabolism and provides a predictable pharmacokinetic profile, making it one of the most commonly prescribed injectable testosterone preparations worldwide for testosterone replacement therapy (TRT). In clinical practice, it has also been used in carefully selected patients with delayed puberty and certain medical conditions associated with androgen deficiency under physician supervision.
Although Testosterone Enanthate is frequently discussed within bodybuilding communities because of its anabolic properties, its primary role remains the treatment of medically diagnosed testosterone deficiency. Current clinical guidelines from organizations such as the Endocrine Society and the American Urological Association (AUA) recommend testosterone therapy only for men with consistent symptoms of hypogonadism and repeatedly confirmed low serum testosterone levels.
Chemical Structure
Testosterone Enanthate consists of a testosterone molecule chemically linked to enanthic acid (heptanoic acid) through esterification at the 17β-hydroxyl group. This structural modification does not alter testosterone’s biological activity after administration; instead, it changes how quickly the hormone is released into circulation.
After intramuscular injection, tissue esterases gradually cleave the ester bond, releasing bioidentical testosterone into the bloodstream. Once liberated from its ester, testosterone interacts with androgen receptors exactly as naturally produced endogenous testosterone does.
Because of this design, Testosterone Enanthate provides sustained hormone delivery for several days rather than requiring daily administration.
Testosterone Ester: Why the Enanthate Ester Exists
The enanthate ester was developed to solve one of the major limitations of native testosterone: its extremely short biological half-life.
Unmodified testosterone is rapidly metabolized, making it impractical for long-term hormone replacement. By attaching an enanthate ester, manufacturers increase the molecule’s lipid solubility, allowing it to remain within muscle tissue after injection and enter the bloodstream gradually over time.
This controlled-release mechanism offers several clinical advantages:
- Longer duration of action than unesterified testosterone.
- Fewer injections compared with short-acting testosterone preparations.
- More stable serum testosterone concentrations.
- Reduced hormonal fluctuations between injections.
- Improved treatment adherence for patients receiving long-term TRT.
These pharmacokinetic characteristics explain why Testosterone Enanthate has remained one of the most widely prescribed injectable testosterone esters for decades.
FDA-Approved Medical Uses
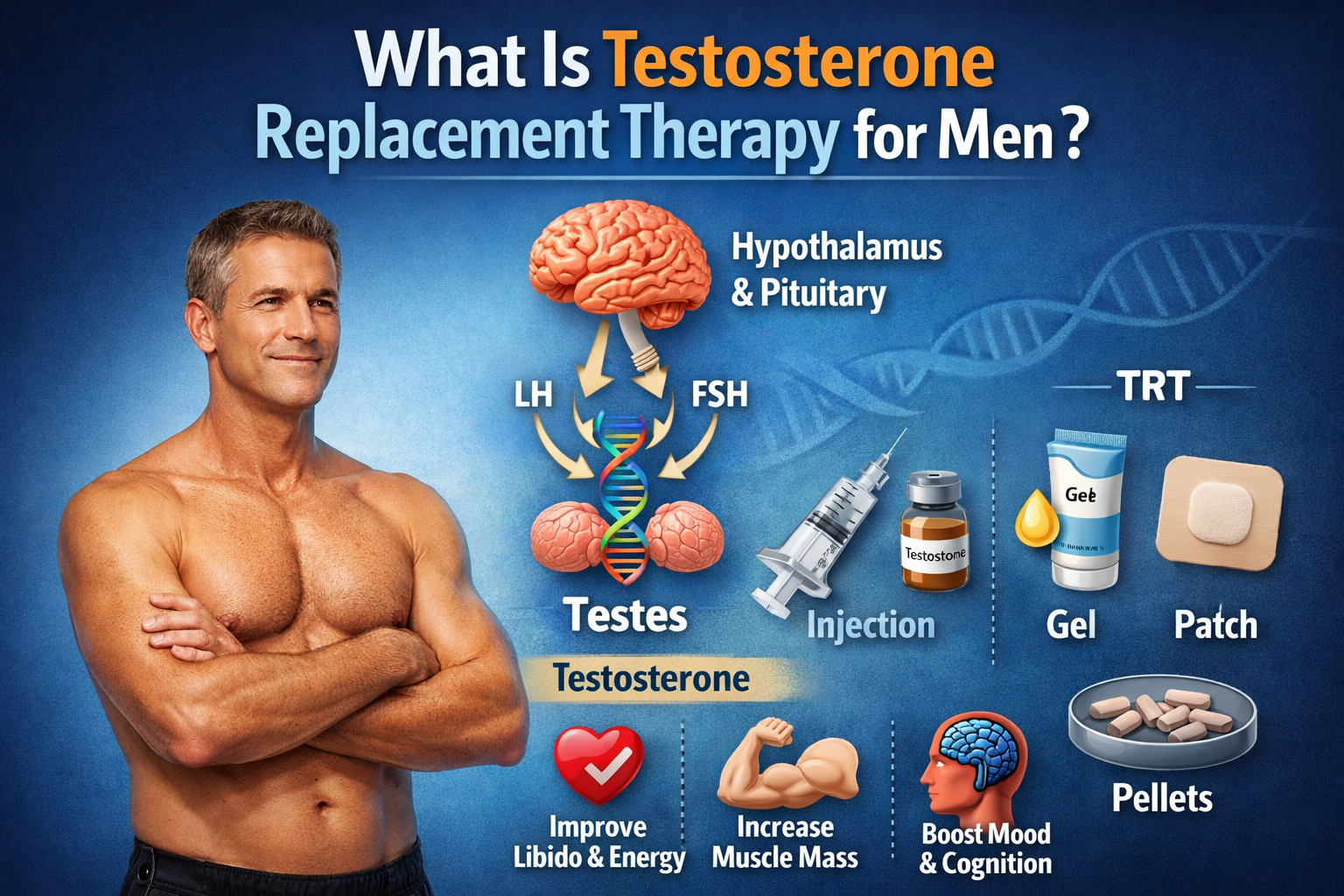
In the United States, Testosterone Enanthate is approved for the treatment of specific medical conditions involving androgen deficiency. Its primary indication is male hypogonadism, where testosterone production is insufficient due to disorders affecting the testes, pituitary gland, or hypothalamus.
Additional approved or historically recognized therapeutic indications include:
- Primary hypogonadism.
- Hypogonadotropic hypogonadism.
- Delayed puberty in carefully selected adolescent males under specialist supervision.
- Certain palliative treatments for metastatic breast cancer in women (historical indication with limited contemporary use).
Testosterone therapy should only be initiated after laboratory confirmation of low testosterone levels combined with compatible clinical symptoms, as recommended by current endocrine guidelines.
Introduction to Testosterone Enanthate Pharmacokinetics
Following intramuscular administration, Testosterone Enanthate is slowly absorbed from the injection site into systemic circulation. Enzymatic hydrolysis gradually separates the testosterone molecule from the enanthate ester, resulting in a prolonged release profile that supports therapeutic testosterone concentrations over several days.
Peak serum testosterone levels typically occur within the first 24 to 48 hours after injection, followed by a gradual decline as the ester continues to release testosterone. Most treatment protocols divide injections every 5 to 7 days or every 7 to 14 days depending on the clinical objective, patient response, and physician preference.
This sustained pharmacokinetic profile is one of the primary reasons Testosterone Enanthate remains a cornerstone medication in testosterone replacement therapy.
Testosterone vs. Testosterone Enanthate: What’s the Difference?
Although the names are often used interchangeably, testosterone and Testosterone Enanthate are not identical compounds.
Testosterone is the naturally occurring androgen hormone produced primarily by the Leydig cells of the testes. It regulates reproductive function, muscle protein synthesis, bone mineral density, erythropoiesis, libido, mood, and numerous metabolic processes.
Testosterone Enanthate, on the other hand, is a pharmaceutical delivery system. The attached enanthate ester temporarily delays hormone release after injection but is removed by enzymes before testosterone becomes biologically active.
In practical terms, the ester influences how long testosterone remains in the body, not how testosterone works once released. After ester cleavage, both endogenous testosterone and testosterone derived from Testosterone Enanthate activate androgen receptors through the same physiological mechanisms.
Clinical Perspective: Why Testosterone Enanthate Is Commonly Used in TRT
From an endocrinology perspective, Testosterone Enanthate has remained one of the preferred injectable therapies for testosterone replacement because it offers an effective balance between treatment efficacy, dosing flexibility, availability, and cost.
Clinical practice has shown that many men with confirmed hypogonadism experience meaningful improvements in symptoms such as fatigue, reduced libido, decreased muscle mass, impaired sexual function, and diminished quality of life after achieving physiological testosterone concentrations through appropriately monitored TRT. However, treatment success depends on individualized dosing, regular laboratory monitoring, and careful management of potential adverse effects rather than simply increasing testosterone levels.
Current clinical guidelines recommend confirming testosterone deficiency with at least two separate morning testosterone measurements, combined with a comprehensive assessment of symptoms before initiating therapy. During treatment, physicians routinely monitor hematocrit, prostate-specific antigen (PSA) when appropriate, lipid profile, liver function, estradiol, and serum testosterone concentrations to optimize efficacy while minimizing risks.
This evidence-based monitoring strategy explains why Testosterone Enanthate continues to be one of the most frequently prescribed injectable testosterone formulations in clinical endocrinology and men’s health practices.
Common Uses of Test Enanthate in Medicine and Sports
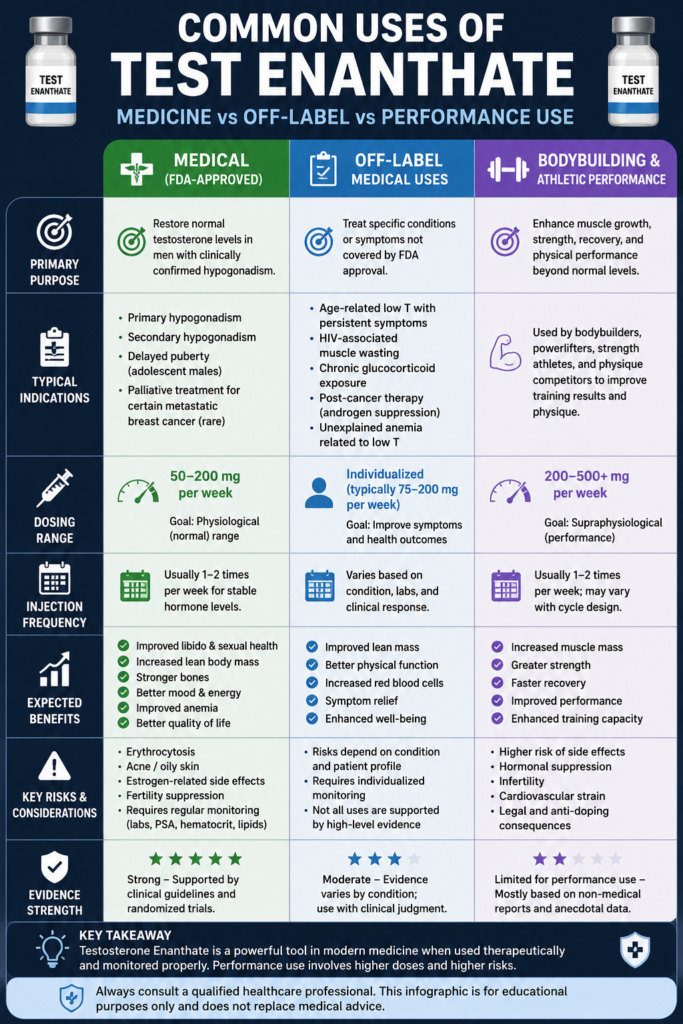
Testosterone Enanthate has been used in clinical practice for more than five decades and remains one of the most frequently prescribed long-acting injectable testosterone preparations worldwide. Its versatility allows it to serve both therapeutic and performance-related purposes, although the objectives, dosing strategies, expected outcomes, and safety considerations differ substantially depending on the context of use.
In medicine, Testosterone Enanthate is prescribed to restore physiological testosterone levels in patients with clinically confirmed androgen deficiency. Treatment is based on evidence-based guidelines, laboratory testing, symptom assessment, and ongoing medical monitoring to ensure that testosterone concentrations remain within the normal physiological range while minimizing adverse effects. Numerous randomized clinical trials have demonstrated improvements in sexual health, lean body mass, bone mineral density, anemia, and quality of life when testosterone replacement therapy (TRT) is appropriately prescribed.
Outside the clinical setting, Testosterone Enanthate has become one of the most widely used anabolic-androgenic steroids among bodybuilders, powerlifters, strength athletes, and physique competitors because of its ability to promote muscle hypertrophy, increase strength, accelerate recovery, and improve training performance. However, these performance-enhancing protocols often involve supraphysiological doses that exceed those recommended for medical treatment, increasing the likelihood of endocrine suppression, cardiovascular complications, infertility, erythrocytosis, and other dose-dependent adverse effects.
Understanding these different applications is essential because the strongest scientific evidence supporting Testosterone Enanthate comes from medically supervised testosterone replacement therapy rather than recreational or competitive performance enhancement. The following sections explain the most common clinical indications, off-label therapeutic applications, and non-medical uses of Testosterone Enanthate while highlighting the current evidence supporting each practice.
FDA-Approved Medical Uses
The primary FDA-approved indication for Testosterone Enanthate is the treatment of male hypogonadism, a condition characterized by inadequate testosterone production resulting from disorders affecting the testes (primary hypogonadism) or dysfunction of the hypothalamic-pituitary axis (secondary hypogonadism). Before initiating therapy, clinicians are advised to confirm consistently low morning serum testosterone concentrations on at least two separate occasions while correlating laboratory findings with compatible clinical symptoms.
Patients diagnosed with hypogonadism frequently report reduced libido, erectile dysfunction, chronic fatigue, loss of muscle mass, increased body fat, decreased bone density, impaired concentration, depressed mood, anemia, and diminished physical performance. Testosterone replacement therapy aims to restore circulating testosterone to physiological levels, thereby improving these symptoms without producing the excessive androgen exposure associated with anabolic steroid abuse.
Historically, Testosterone Enanthate has also been approved for carefully selected cases of delayed puberty in adolescent males under specialist supervision and has been used as palliative therapy for certain forms of metastatic breast cancer in women, although these indications are far less common today due to advances in alternative treatments.
Current recommendations from the Endocrine Society, American Urological Association (AUA), and other international endocrine organizations emphasize that testosterone therapy should never be initiated solely on the basis of laboratory values. Instead, treatment decisions should combine biochemical confirmation of testosterone deficiency with a comprehensive clinical evaluation, patient history, physical examination, and assessment of potential contraindications.
Off-Label Medical Uses
Although FDA-approved indications remain relatively limited, physicians may prescribe Testosterone Enanthate for several off-label medical applications when supported by sound clinical judgment and appropriate monitoring.
One of the most common off-label uses involves the management of symptomatic age-related testosterone deficiency in carefully selected men after exclusion of reversible causes such as obesity, medication effects, chronic illness, sleep apnea, or uncontrolled metabolic disease. While age alone is not considered an indication for testosterone therapy, some patients with persistent symptoms and consistently low testosterone concentrations may benefit from individualized treatment plans.
Testosterone Enanthate may also be considered in selected patients with HIV-associated muscle wasting, chronic glucocorticoid exposure, prolonged androgen suppression following certain cancer therapies, or severe unexplained anemia associated with testosterone deficiency. In these situations, treatment is intended to improve lean body mass, physical function, erythropoiesis, and overall quality of life rather than simply increasing serum testosterone levels.
Because evidence supporting off-label applications varies considerably between medical conditions, clinicians typically perform regular monitoring of hematocrit, prostate-specific antigen (PSA) when appropriate, lipid profile, liver function, cardiovascular risk factors, and serum testosterone concentrations throughout treatment. Shared decision-making and individualized risk-benefit assessment remain essential components of responsible testosterone prescribing.
Bodybuilding and Athletic Performance
Beyond its established role in clinical endocrinology, Testosterone Enanthate has become one of the foundational anabolic compounds used in bodybuilding and strength sports. Its relatively long half-life, predictable release profile, widespread availability, and potent anabolic effects make it one of the most commonly selected testosterone esters for both novice and experienced athletes.
Within bodybuilding, Testosterone Enanthate is used primarily to promote muscle hypertrophy, increase strength, enhance nitrogen retention, accelerate recovery between training sessions, improve glycogen storage, and support greater training intensity. These physiological effects result from testosterone’s ability to activate androgen receptors, stimulate muscle protein synthesis, increase insulin-like growth factor-1 (IGF-1) signaling, and promote satellite cell activation involved in muscle repair and growth.
Unlike testosterone replacement therapy, bodybuilding protocols frequently employ doses several times higher than normal physiological replacement levels. Although higher androgen exposure may produce greater anabolic responses, it also substantially increases the risk of adverse effects, including suppression of endogenous testosterone production, infertility, gynecomastia, acne, androgenic alopecia, elevated hematocrit, dyslipidemia, hypertension, and long-term cardiovascular complications.
Competitive athletes should also recognize that Testosterone Enanthate is classified as a prohibited substance by the World Anti-Doping Agency (WADA) and most professional sporting organizations. Detection methods are capable of identifying exogenous testosterone administration through isotope ratio mass spectrometry (IRMS) and other advanced anti-doping techniques, making unauthorized use incompatible with drug-tested competition.
Although Testosterone Enanthate remains one of the most researched anabolic-androgenic steroids, its use for physique or performance enhancement should not be considered equivalent to medically supervised testosterone replacement therapy. Clinical treatment seeks to restore normal endocrine function, whereas performance-enhancing protocols intentionally exceed physiological hormone concentrations and therefore carry significantly greater health risks.
Who Is an Ideal Candidate for Testosterone Enanthate Therapy?
The ideal candidate for Testosterone Enanthate therapy is an adult male with persistent symptoms of testosterone deficiency and repeatedly confirmed low morning serum testosterone concentrations measured using reliable laboratory methods. Diagnosis should never rely on symptoms alone or a single laboratory value, as testosterone levels naturally fluctuate according to circadian rhythm, illness, nutritional status, medication use, and other physiological factors.
Patients who may benefit from testosterone replacement therapy commonly present with symptoms such as reduced libido, erectile dysfunction, decreased spontaneous morning erections, chronic fatigue, loss of muscle mass, increased abdominal fat, reduced bone mineral density, impaired concentration, depressed mood, infertility associated with hypogonadism, or unexplained anemia linked to androgen deficiency.
Before initiating therapy, clinicians should conduct a comprehensive medical evaluation that includes measurement of total testosterone, free testosterone when indicated, luteinizing hormone (LH), follicle-stimulating hormone (FSH), complete blood count (CBC), prostate-specific antigen (PSA) in appropriate patients, liver function tests, lipid profile, and cardiovascular risk assessment. Identifying reversible causes of low testosterone—including obesity, obstructive sleep apnea, uncontrolled diabetes, thyroid disorders, chronic illness, excessive alcohol consumption, or medication effects—is equally important before considering lifelong hormone replacement.
Conversely, Testosterone Enanthate is generally not recommended for men with normal endogenous testosterone levels, individuals actively attempting to preserve fertility, patients with untreated prostate or breast cancer, uncontrolled polycythemia, severe untreated obstructive sleep apnea, or those with significant cardiovascular instability until these conditions have been appropriately evaluated and managed. Careful patient selection remains one of the most important factors influencing both the safety and long-term success of testosterone replacement therapy.
How Test Enanthate Works in the Body
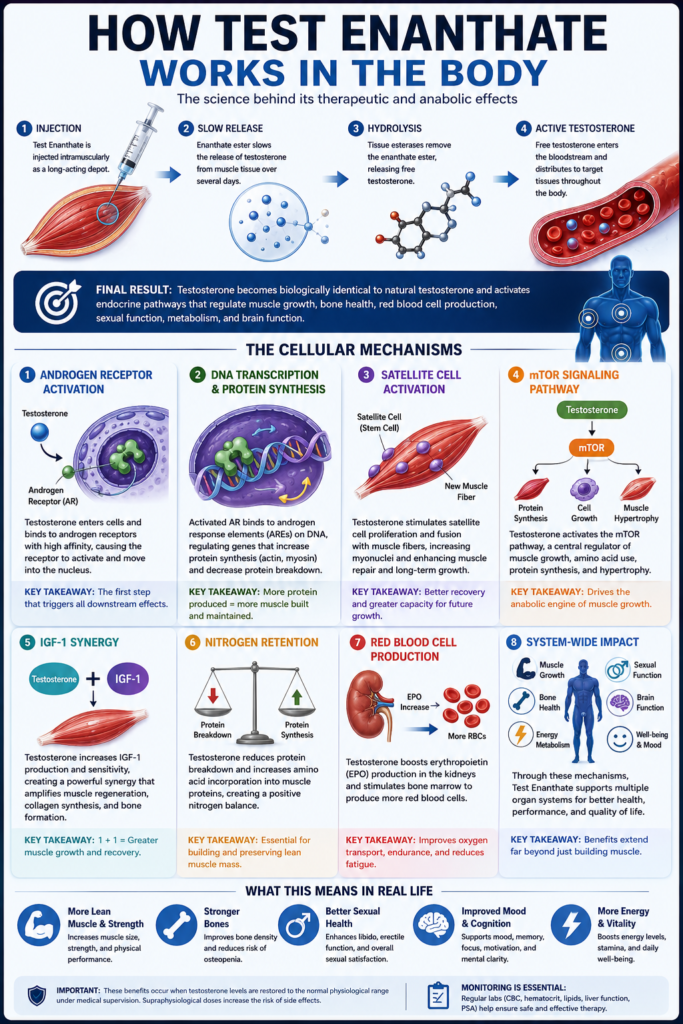
Testosterone Enanthate exerts its therapeutic and anabolic effects through a complex series of physiological processes that begin immediately after intramuscular injection and continue as the drug is gradually released into circulation. Unlike oral medications that are absorbed rapidly through the gastrointestinal tract, Testosterone Enanthate is formulated as a long-acting depot injection. The attached enanthate ester slows the release of testosterone from muscle tissue, allowing hormone concentrations to remain elevated for several days rather than only a few hours.
Once the ester is enzymatically removed, the released testosterone becomes biologically identical to the hormone naturally produced by the testes. From that point forward, it participates in the same endocrine pathways responsible for regulating muscle protein synthesis, bone remodeling, red blood cell production, sexual function, metabolism, and numerous neurological processes. These widespread physiological actions explain why testosterone deficiency affects multiple organ systems simultaneously and why restoring normal hormone concentrations can improve both physical and psychological health.
The biological activity of Testosterone Enanthate extends far beyond simply increasing circulating testosterone levels. It influences gene expression, activates anabolic signaling pathways, stimulates muscle regeneration, enhances oxygen transport, and regulates numerous metabolic functions throughout the body. Understanding these cellular mechanisms helps explain why Testosterone Enanthate has become one of the most extensively studied medications in testosterone replacement therapy and one of the most widely recognized anabolic compounds in sports medicine.
Mechanism of Action: How Testosterone Enanthate Works at the Cellular Level
After intramuscular administration, Testosterone Enanthate is gradually hydrolyzed by tissue esterases, releasing free testosterone into the bloodstream. This testosterone then diffuses through cell membranes and binds to the androgen receptor (AR), an intracellular nuclear receptor expressed in skeletal muscle, bone, adipose tissue, reproductive organs, the central nervous system, and numerous other tissues.
Once activated, the androgen receptor initiates a cascade of molecular events that regulate muscle growth, tissue repair, metabolism, reproductive function, and red blood cell production. These coordinated biological responses explain both the therapeutic effects observed during testosterone replacement therapy (TRT) and the anabolic effects associated with athletic performance enhancement.
Androgen Receptor Activation: The First Step of Testosterone Action
The androgen receptor is the primary molecular target of testosterone. After entering the cell, testosterone binds to this receptor with high affinity, triggering a conformational change that activates the receptor and allows it to migrate into the cell nucleus.
Inside the nucleus, the activated androgen receptor binds to androgen response elements (AREs) located within DNA, regulating the expression of hundreds of genes involved in muscle protein synthesis, bone remodeling, erythropoiesis, reproductive health, and energy metabolism.
Because androgen receptors are widely distributed throughout the body, Testosterone Enanthate produces systemic effects that extend well beyond skeletal muscle, influencing nearly every organ system that depends on normal androgen signaling.
DNA Transcription and Muscle Protein Synthesis
One of testosterone’s most important physiological actions occurs at the genetic level.
Following androgen receptor activation, testosterone stimulates DNA transcription of anabolic genes responsible for producing structural proteins such as actin and myosin while simultaneously reducing the activity of catabolic pathways involved in muscle protein degradation.
This increase in muscle protein synthesis creates a positive protein balance, allowing skeletal muscle to repair damaged fibers, adapt to resistance training, and progressively increase lean muscle mass. Clinical research consistently demonstrates that restoring physiological testosterone levels significantly enhances body composition in men with testosterone deficiency.
Satellite Cells: How Testosterone Repairs and Builds Muscle
Satellite cells are specialized muscle stem cells responsible for repairing damaged muscle tissue and supporting long-term muscle hypertrophy.
Testosterone stimulates satellite cell proliferation, differentiation, and fusion with existing muscle fibers, increasing the number of myonuclei available to support ongoing protein synthesis. This process allows muscles to recover more efficiently from training while improving their capacity for future growth.
Studies suggest that enhanced satellite cell activity is one of the primary mechanisms responsible for the gradual increases in lean muscle mass observed during long-term testosterone replacement therapy.
mTOR Signaling: Why Testosterone Stimulates Muscle Growth
The mechanistic target of rapamycin (mTOR) pathway is one of the body’s most important regulators of muscle growth.
Testosterone activates mTOR signaling through androgen receptor-mediated pathways, stimulating cellular growth, amino acid utilization, muscle protein synthesis, and muscle fiber hypertrophy. This anabolic signaling pathway plays a central role in the body’s adaptation to resistance exercise and is considered one of the primary biological mechanisms responsible for testosterone-induced increases in skeletal muscle mass.
When combined with progressive resistance training and adequate dietary protein intake, activation of the mTOR pathway contributes significantly to long-term improvements in strength and muscle development.
IGF-1 and Testosterone: How They Work Together
Testosterone also enhances the production and activity of insulin-like growth factor-1 (IGF-1), a hormone that plays an essential role in muscle regeneration, tissue repair, collagen synthesis, and bone formation.
Rather than functioning independently, testosterone and IGF-1 work synergistically to maximize anabolic signaling. Increased local IGF-1 expression within skeletal muscle amplifies satellite cell activation, accelerates muscle recovery following exercise, and supports continued muscle hypertrophy over time.
This interaction between testosterone and IGF-1 is considered one of the key mechanisms underlying the improvements in muscle mass and physical performance observed in hypogonadal men receiving testosterone replacement therapy.
Nitrogen Retention: Why Testosterone Creates an Anabolic Environment
Maintaining a positive nitrogen balance is essential for preserving and building skeletal muscle.
Testosterone promotes nitrogen retention by reducing protein breakdown while increasing amino acid incorporation into newly synthesized muscle proteins. This anabolic environment supports muscle maintenance during periods of calorie restriction and facilitates greater muscle growth during resistance training.
Improved nitrogen retention has long been recognized as one of testosterone’s fundamental physiological effects and remains an important contributor to the increases in lean body mass observed during testosterone replacement therapy.
How Testosterone Increases Red Blood Cell Production
In addition to its anabolic effects, Testosterone Enanthate stimulates erythropoiesis, the process responsible for producing red blood cells within the bone marrow.
Testosterone increases renal production of erythropoietin (EPO) while directly stimulating erythroid precursor cells, leading to higher hemoglobin concentrations, increased hematocrit, and improved oxygen-carrying capacity.
Greater oxygen delivery to skeletal muscles can improve exercise tolerance, reduce fatigue, and enhance overall physical performance in men with testosterone deficiency. However, because excessive erythrocytosis is a recognized complication of testosterone therapy, routine monitoring of complete blood count (CBC) and hematocrit is recommended throughout treatment.
Testosterone Enanthate Pharmacokinetics: Absorption, Half-Life, Metabolism, and Elimination
The pharmacokinetic profile of Testosterone Enanthate determines how quickly the medication enters the bloodstream, how long it remains active, and how frequently injections are required to maintain stable testosterone levels.
Unlike unesterified testosterone, which is rapidly metabolized within hours, Testosterone Enanthate is formulated as a long-acting depot injection. The attached enanthate ester delays hormone release, providing sustained testosterone exposure for several days while minimizing the need for frequent injections.
Understanding its absorption, metabolism, half-life, and elimination helps physicians optimize testosterone replacement therapy by selecting dosing schedules that maintain stable serum testosterone concentrations and reduce hormonal fluctuations associated with peaks and troughs.
Absorption: How Testosterone Enanthate Enters the Bloodstream
Following intramuscular injection, Testosterone Enanthate forms a depot within muscle tissue. Because the molecule is highly lipophilic, it diffuses slowly into surrounding capillaries over several days.
This gradual absorption produces a controlled increase in circulating testosterone concentrations and contributes to the medication’s prolonged duration of action.
Although injection site, muscle blood flow, and body composition may slightly influence absorption, Testosterone Enanthate generally demonstrates predictable pharmacokinetics when administered correctly.
Metabolism: How Testosterone Enanthate Is Processed in the Body
Once absorbed into circulation, plasma esterases rapidly hydrolyze the enanthate ester, releasing free testosterone.
The liberated testosterone follows the body’s normal metabolic pathways. It may be converted into dihydrotestosterone (DHT) by the enzyme 5-alpha reductase or aromatized into estradiol by aromatase enzymes. Ultimately, testosterone is metabolized primarily in the liver into inactive metabolites, including androsterone and etiocholanolone, which are excreted through the kidneys.
Importantly, the enanthate ester itself has no hormonal activity; its only function is to regulate the rate at which testosterone is released after injection.
Half-Life of Testosterone Enanthate
The terminal elimination half-life of intramuscular Testosterone Enanthate is generally reported to range between 4.5 and 5 days, although some pharmacokinetic studies have observed values approaching 7 days depending on formulation and individual patient characteristics.
Because serum testosterone levels gradually decline after injection, many endocrinologists recommend administering Testosterone Enanthate every 5 to 7 days or dividing the weekly dose into two smaller injections to maintain more stable hormone concentrations and reduce fluctuations between peak and trough levels.
Peak Testosterone Levels After Injection
Serum testosterone concentrations typically reach their highest levels approximately 24 to 48 hours after intramuscular administration.
Following this initial peak, hormone concentrations decline gradually as testosterone continues to be released from the intramuscular depot. Larger injection intervals often produce greater hormonal fluctuations, whereas more frequent injections using smaller doses generally provide smoother and more physiologic testosterone profiles.
When Does Testosterone Enanthate Reach Steady State?
With consistent dosing, Testosterone Enanthate gradually reaches steady-state concentrations, a point at which the amount of testosterone administered equals the amount eliminated between injections.
For most patients, relatively stable hormone levels are achieved after approximately 4 to 6 weeks of regular therapy. Reaching steady state is clinically important because laboratory monitoring, symptom evaluation, and dosage adjustments become more reliable once testosterone concentrations have stabilized.
Why Injection Frequency Matters
Injection frequency plays a critical role in maintaining stable testosterone concentrations throughout treatment. While some traditional protocols recommend injections every one to two weeks, many modern TRT specialists prefer administering smaller doses once or twice weekly to minimize hormonal fluctuations and improve symptom control.
More frequent injections often result in lower peak testosterone levels, higher trough concentrations, and greater hormonal stability, which may reduce side effects such as mood swings, energy fluctuations, and excessive estradiol production. Individual injection schedules should always be tailored according to laboratory results, clinical response, patient preference, and physician recommendations to achieve the best balance between efficacy, safety, and long-term treatment adherence.
Dosage Guidelines and Administration
Testosterone Enanthate dosage should always be individualized according to the patient’s diagnosis, baseline testosterone levels, symptoms, age, body composition, treatment goals, and laboratory response. In medical settings, the objective is not to push testosterone as high as possible, but to restore serum testosterone into a healthy physiological range while minimizing adverse effects such as erythrocytosis, estrogen imbalance, acne, infertility, and cardiovascular strain.
Because Testosterone Enanthate is a long-acting injectable ester, dosing schedules are usually based on its pharmacokinetic profile, including absorption rate, half-life, peak serum levels, and trough concentrations before the next injection. More frequent, smaller injections often provide more stable hormone levels than large, infrequent doses.
TRT Dosage: Testosterone Enanthate for Testosterone Replacement Therapy
For testosterone replacement therapy, Testosterone Enanthate is commonly prescribed in the range of 50–200 mg per week, depending on the patient’s laboratory results and clinical response. Some protocols use 100–200 mg every 1–2 weeks, but many clinicians prefer smaller weekly or twice-weekly injections to reduce hormonal fluctuations.
The goal of TRT is to restore testosterone into the mid-normal physiological range, not to achieve supraphysiological levels. Follow-up bloodwork is typically used to adjust dosage based on total testosterone, free testosterone, hematocrit, estradiol, lipids, PSA when appropriate, and symptom improvement.
Hypogonadism Dosage: Medical Use in Testosterone Deficiency
In men with primary or secondary hypogonadism, Testosterone Enanthate is used to replace insufficient endogenous testosterone production. The dosage depends on whether the condition is caused by testicular failure, pituitary dysfunction, hypothalamic dysfunction, aging-related androgen deficiency, or another endocrine disorder.
A typical medical approach may begin with a conservative dose, followed by laboratory reassessment after several weeks once serum testosterone reaches a more stable pattern. Physicians may increase, reduce, or divide the dose depending on trough testosterone levels, symptom response, hematocrit, estradiol-related symptoms, and adverse effects.
Bodybuilding Dosage: Performance-Enhancing Use
In bodybuilding and performance-enhancement settings, Testosterone Enanthate is often used at doses higher than medical replacement levels. Non-medical protocols commonly range from 200–500 mg per week, while some experienced users may exceed this range.
However, supraphysiological dosing increases the risk of testosterone suppression, infertility, gynecomastia, acne, hair loss, elevated hematocrit, blood pressure changes, dyslipidemia, and long-term cardiovascular complications. Unlike TRT, bodybuilding use is not designed to restore normal hormone levels; it intentionally raises androgen exposure beyond physiological ranges, which makes medical monitoring especially important.
Injection Frequency: How Often Is Testosterone Enanthate Injected?
Testosterone Enanthate is commonly injected once weekly or divided into two smaller injections per week. Although older protocols often used injections every 10–14 days, this approach may produce higher peaks and lower troughs, leading to mood changes, energy fluctuations, libido changes, or estrogen-related symptoms in some patients.
Many modern TRT protocols favor weekly or twice-weekly dosing because it can help maintain more consistent testosterone levels. Injection frequency should be based on bloodwork, symptom control, side effects, and physician guidance.
Missed Dose: What Happens If You Miss a Testosterone Enanthate Injection?
If a Testosterone Enanthate injection is missed, the next step depends on how late the dose is and the prescribed schedule. Because Testosterone Enanthate has a relatively long half-life, missing a dose by a short period usually does not cause an immediate hormonal crash, but repeated missed doses can lead to unstable testosterone levels and symptom recurrence.
Patients should not double the next injection without medical guidance. In most clinical situations, the missed dose is taken as soon as remembered, or the patient resumes the regular schedule depending on how close it is to the next planned injection.
Testosterone Enanthate Dosage Table
| Purpose | Dose | Frequency | Evidence |
|---|---|---|---|
| TRT / testosterone replacement therapy | 50–200 mg per week | Weekly or split 2x weekly | Supported by endocrine and urology guidelines for confirmed hypogonadism |
| Male hypogonadism | Individualized, often 75–200 mg per week | Weekly, every 10 days, or every 2 weeks depending on labs | Used to restore physiological testosterone levels |
| Delayed puberty | Specialist-directed only | Physician-determined | Used only under pediatric endocrinology supervision |
| Bodybuilding / performance enhancement | Commonly 200–500 mg per week | Usually weekly or split 2x weekly | Based largely on non-medical practice, not standard clinical guidelines |
| More stable TRT protocol | Smaller divided doses | 2x weekly | May reduce peak-and-trough fluctuations |
| Missed dose management | Do not double dose | Resume or adjust based on timing | Should follow prescribing clinician’s instructions |
Potential Side Effects and Risks
While Test Enanthate offers numerous benefits, it’s important to be aware of the potential side effects and risks associated with its use. Common side effects include acne, oily skin, and hair loss, which are often attributed to the hormone’s androgenic properties. These side effects can vary in severity and may be more pronounced in individuals who are genetically predisposed to these conditions.
Another potential risk is the suppression of natural testosterone production. When exogenous testosterone is introduced into the body, it can signal the hypothalamus and pituitary gland to reduce or stop the production of endogenous testosterone. This can lead to testicular atrophy and decreased sperm production, which may impact fertility. Post-cycle therapy (PCT) is often recommended to help restore natural hormone levels after discontinuing Test Enanthate use.
Cardiovascular risks are also a concern, as testosterone can affect cholesterol levels and increase the risk of hypertension and cardiovascular disease. Regular monitoring of blood pressure, cholesterol levels, and overall cardiovascular health is essential for individuals using Test Enanthate. It’s also important to be aware of the potential for liver toxicity, particularly with higher doses or prolonged use. Liver function tests should be conducted periodically to ensure the liver is functioning properly.
Best Practices for Using Test Enanthate Safely
To maximize the benefits of Test Enanthate while minimizing the risks, it’s important to follow best practices for its use. First and foremost, consulting with a healthcare professional before starting Test Enanthate is crucial. A healthcare provider can assess individual health status, determine the appropriate dosage, and monitor for potential side effects. Regular follow-up appointments are essential for ongoing assessment and adjustment of the treatment plan.
Maintaining a healthy lifestyle is also important for individuals using Test Enanthate. A balanced diet rich in nutrients, regular exercise, and adequate sleep can help support overall health and enhance the effects of testosterone therapy. Reducing alcohol consumption and avoiding recreational drugs can further minimize the risk of adverse effects.
Proper injection technique is another key aspect of safe Test Enanthate use. Using sterile equipment, rotating injection sites, and following proper hygiene practices can help prevent infections and other complications. Additionally, individuals should be educated on how to recognize signs of adverse reactions, such as pain, swelling, or redness at the injection site, and seek medical attention if necessary.
Conclusion: Making Informed Decisions about Test Enanthate
In conclusion, Test Enanthate offers a range of benefits for both medical and performance enhancement purposes. Its ability to promote muscle growth, fat loss, and overall physical vitality makes it a valuable tool for individuals seeking to improve their health and fitness. However, it’s important to approach its use with caution and awareness of the potential risks and side effects.
Consulting with a healthcare professional, following proper dosage and administration guidelines, and maintaining a healthy lifestyle are key factors in using Test Enanthate safely and effectively. Being aware of the legal considerations and regulations governing its use is also essential to avoid legal complications and ensure ethical compliance.
Ultimately, making informed decisions about Test Enanthate requires a thorough understanding of its benefits, uses, and best practices. By staying educated and proactive, individuals can unlock the potential of Test Enanthate while minimizing the risks and maximizing the benefits for their fitness journey and overall well-being.
Frequently Asked Questions About Test Enanthate
Is Test Enanthate the Same as Testosterone Enanthate?
Yes. Test Enanthate is the abbreviated name commonly used for Testosterone Enanthate. Both terms refer to the same long-acting injectable testosterone ester used in testosterone replacement therapy and widely discussed in bodybuilding. After injection, the enanthate ester is gradually removed by enzymes, releasing bioidentical testosterone into the bloodstream.
How Long Does Test Enanthate Stay in Your System?
Test Enanthate has an average elimination half-life of approximately 4.5 to 5 days, although some studies report values closer to 7 days depending on formulation, injection site, and individual metabolism. Because the compound remains active for several days, it is commonly injected once weekly or divided into two smaller weekly injections.
How Long Does It Take for Test Enanthate to Start Working?
Test Enanthate may begin improving energy, mood, libido, and general well-being within the first 2 to 4 weeks in men with testosterone deficiency. Changes in lean muscle mass, strength, body composition, and bone mineral density usually take longer and may require several months of consistent therapy.
Can Test Enanthate Be Used for TRT?
Yes. Test Enanthate is one of the most commonly prescribed injectable medications for testosterone replacement therapy. It is generally used in men with confirmed hypogonadism, persistent symptoms of testosterone deficiency, and repeatedly low morning testosterone levels. Treatment should include regular medical supervision and laboratory monitoring.
Can Test Enanthate Help Build Muscle?
Yes. Test Enanthate can support muscle growth by increasing androgen receptor activation, muscle protein synthesis, nitrogen retention, satellite cell activity, IGF-1 signaling, and mTOR pathway activity. In men with low testosterone, these mechanisms may improve lean body mass, especially when combined with resistance training and adequate nutrition.
How Often Should Test Enanthate Be Injected?
Test Enanthate is commonly injected once weekly or divided into two smaller injections per week. More frequent dosing may help maintain stable testosterone levels and reduce hormonal fluctuations between peak and trough concentrations. The ideal schedule depends on bloodwork, symptoms, side effects, and physician guidance.
Does Test Enanthate Increase Estrogen Levels?
Yes. Some testosterone from Test Enanthate can convert into estradiol through the aromatase enzyme. Estradiol is necessary for bone health, libido, and cardiovascular function, but excessive estrogen may contribute to water retention, breast tenderness, mood changes, or gynecomastia in susceptible individuals.
Does Test Enanthate Affect Fertility?
Yes. Test Enanthate can suppress the hypothalamic-pituitary-gonadal axis, reducing luteinizing hormone and follicle-stimulating hormone. This can lower natural testosterone production and significantly reduce sperm production during treatment. Men who want to preserve fertility should discuss alternatives with a physician before starting therapy.
What Blood Tests Are Recommended With Test Enanthate?
Common blood tests during Test Enanthate therapy include total testosterone, free testosterone when indicated, complete blood count, hematocrit, estradiol, lipid profile, liver enzymes, and prostate-specific antigen when clinically appropriate. These tests help evaluate both treatment effectiveness and potential side effects.
Is Test Enanthate Safe for Long-Term Use?
Test Enanthate can be used long term when prescribed for medically confirmed testosterone deficiency and monitored according to clinical guidelines. Long-term safety depends on proper dosing, regular bloodwork, hematocrit monitoring, cardiovascular risk assessment, prostate health evaluation when appropriate, and individualized follow-up care.
References
Bhasin, S., Brito, J. P., Cunningham, G. R., Hayes, F. J., Hodis, H. N., Matsumoto, A. M., Snyder, P. J., Swerdloff, R. S., Wu, F. C. W., & Yialamas, M. A. (2018). Testosterone therapy in men with hypogonadism: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 103(5), 1715–1744. https://doi.org/10.1210/jc.2018-00229
https://academic.oup.com/jcem/article/103/5/1715/4939465
Mulhall, J. P., Trost, L. W., Brannigan, R. E., Kurtz, E. G., Redmon, J. B., Chiles, K. A., Lightner, D. J., Miner, M. M., Murad, M. H., Nelson, C. J., Platz, E. A., Ramanathan, L. V., & Lewis, R. W. (2018). Evaluation and management of testosterone deficiency: American Urological Association guideline. The Journal of Urology, 200(2), 423–432.
https://www.auanet.org/guidelines-and-quality/guidelines/testosterone-deficiency-guideline
Bhasin, S., Woodhouse, L., Casaburi, R., Singh, A. B., Bhasin, D., Berman, N., Chen, X., Yarasheski, K. E., Magliano, L., Dzekov, C., Dzekov, J., Bross, R., Phillips, J., Sinha-Hikim, I., Shen, R., & Storer, T. W. (2001). Testosterone dose-response relationships in healthy young men. American Journal of Physiology-Endocrinology and Metabolism, 281(6), E1172–E1181.
https://doi.org/10.1152/ajpendo.2001.281.6.E1172
https://journals.physiology.org/doi/10.1152/ajpendo.2001.281.6.E1172
Snyder, P. J., Bhasin, S., Cunningham, G. R., Matsumoto, A. M., Stephens-Shields, A. J., Cauley, J. A., Gill, T. M., Barrett-Connor, E., Swerdloff, R. S., Wang, C., et al. (2016). Effects of testosterone treatment in older men. The New England Journal of Medicine, 374(7), 611–624.
https://doi.org/10.1056/NEJMoa1506119
https://www.nejm.org/doi/full/10.1056/NEJMoa1506119
Cunningham, G. R., Stephens-Shields, A. J., Rosen, R. C., Wang, C., Bhasin, S., Matsumoto, A. M., Parsons, J. K., Gill, T. M., Molitch, M. E., Farrar, J. T., Cella, D., Barrett-Connor, E., Cauley, J. A., Crandall, J. P., Ensrud, K. E., Lewis, C. E., & Snyder, P. J. (2016). Testosterone treatment and sexual function in older men with low testosterone levels. The Journal of Clinical Endocrinology & Metabolism, 101(8), 3096–3104.
https://doi.org/10.1210/jc.2016-1645
https://academic.oup.com/jcem/article/101/8/3096/2804769
Snyder, P. J., Kopperdahl, D. L., Stephens-Shields, A. J., Ellenberg, S. S., Cauley, J. A., Ensrud, K. E., Lewis, C. E., Barrett-Connor, E., Schwartz, A. V., Lee, D. C., et al. (2017). Effect of testosterone treatment on volumetric bone density and strength in older men with low testosterone: A controlled clinical trial. JAMA Internal Medicine, 177(4), 471–479.
https://doi.org/10.1001/jamainternmed.2016.9539
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2604138
Roy, C. N., Snyder, P. J., Stephens-Shields, A. J., Artz, A. S., Bhasin, S., Cohen, H. J., Farrar, J. T., Gill, T. M., Zeldow, B., Cella, D., Barrett-Connor, E., Cauley, J. A., Crandall, J. P., Cunningham, G. R., Ensrud, K. E., Lewis, C. E., & Matsumoto, A. M. (2017). Association of testosterone levels with anemia in older men: A controlled clinical trial. JAMA Internal Medicine, 177(4), 480–490.
https://doi.org/10.1001/jamainternmed.2016.9540
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2604139
Pencina, K. M., Travison, T. G., Artz, A. S., Bhasin, S., Snyder, P. J., Storer, T. W., & Basaria, S. (2023). Efficacy of testosterone replacement therapy in correcting anemia in men with hypogonadism. JAMA Network Open, 6(10), e2340030.
https://doi.org/10.1001/jamanetworkopen.2023.40030
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2811115
Lincoff, A. M., Bhasin, S., Flevaris, P., Mitchell, L. M., Basaria, S., Boden, W. E., Cunningham, G. R., Granger, C. B., Khera, M., Thompson, I. M., Wang, C., Wolski, K., Snabes, M. C., & Nissen, S. E. (2023). Cardiovascular safety of testosterone-replacement therapy. The New England Journal of Medicine, 389(2), 107–117.
https://doi.org/10.1056/NEJMoa2215025
https://www.nejm.org/doi/full/10.1056/NEJMoa2215025
Basaria, S., Harman, S. M., Travison, T. G., Hodis, H., Tsitouras, P., Budoff, M., Pencina, K., Vita, J., & Bhasin, S. (2024). Testosterone therapy in older men: Clinical implications of recent randomized placebo-controlled trials. European Journal of Endocrinology, 191(1), R22–R33.
https://doi.org/10.1093/ejendo/lvae082
https://academic.oup.com/ejendo/article/191/1/R22/7698939
Patel, A. S., Leong, J. Y., Ramos, L., & Ramasamy, R. (2025). Testosterone replacement therapy and spermatogenesis in men with hypogonadism. Nature Reviews Urology.
https://doi.org/10.1038/s41585-025-01032-8
https://www.nature.com/articles/s41585-025-01032-8
Pastuszak, A. W., Gittelman, M., Tursi, J. P., Jaffe, J. S., Schofield, D., & Miner, M. M. (2022). Pharmacokinetics of testosterone therapies in relation to diurnal variation of serum testosterone levels as men age. Andrology, 10(6), 1140–1152.
https://doi.org/10.1111/andr.13193
https://pmc.ncbi.nlm.nih.gov/articles/PMC9293229/
Kaminetsky, J., Jaffe, J. S., Swerdloff, R. S., Wang, C., & Morgentaler, A. (2015). Pharmacokinetic profile of subcutaneous testosterone enanthate delivered via a novel autoinjector: A phase II study. Sexual Medicine, 3(4), 269–279.
https://doi.org/10.1002/sm2.86
https://academic.oup.com/smoa/article/3/4/269/6956268
Anawalt, B. D., & Matsumoto, A. M. (2018). Evaluation and treatment of male hypogonadism. JAMA, 319(9), 914–925.
https://doi.org/10.1001/jama.2018.0429
https://jamanetwork.com/journals/jama/fullarticle/2675569
Hackett, G., Kirby, M., Edwards, D., Jones, T. H., Wylie, K., Ossei-Gerning, N., David, J., & Muneer, A. (2022). Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clinical Endocrinology, 96(2), 200–219.
https://doi.org/10.1111/cen.14633
https://onlinelibrary.wiley.com/doi/10.1111/cen.14633
Albano, G. D., Amico, F., Cocimano, G., Liberto, A., Maglietta, F., Esposito, M., Rosi, G. L., Di Nunno, N., Salerno, M., & Montana, A. (2021). Adverse effects of anabolic-androgenic steroids: A literature review. Healthcare, 9(1), 97.
https://doi.org/10.3390/healthcare9010097
https://pmc.ncbi.nlm.nih.gov/articles/PMC7832337/
U.S. Food and Drug Administration. (2025). XYOSTED® (testosterone enanthate) injection: Prescribing information.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/209863s020lbl.pdf
National Library of Medicine. (2024). DailyMed: Testosterone Enanthate Injection, USP.
https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=e89d6458-428c-4256-97a3-f1fa851293c1
World Anti-Doping Agency. (2025). The 2025 Prohibited List: International Standard.
https://www.wada-ama.org/en/prohibited-list
Author
Written by Jonathan E. Carter, MSc, CSCS
Medical Research Writer | Exercise Physiologist | Strength & Conditioning Specialist
Jonathan E. Carter is a medical research writer specializing in endocrinology, testosterone replacement therapy (TRT), exercise physiology, anabolic pharmacology, and evidence-based sports medicine. He has spent more than a decade analyzing peer-reviewed clinical research related to male hormone optimization, skeletal muscle physiology, aging, and performance science.
His editorial work focuses on translating complex scientific literature into medically accurate, easy-to-understand educational content for healthcare professionals, coaches, and individuals seeking reliable information about testosterone deficiency, hormone replacement therapy, and anabolic-androgenic steroids.
Jonathan develops every article using current evidence from high-impact medical journals, including The New England Journal of Medicine, JAMA, The Journal of Clinical Endocrinology & Metabolism, European Journal of Endocrinology, Nature Reviews Urology, and official clinical practice guidelines published by the Endocrine Society, American Urological Association (AUA), and European Association of Urology (EAU).
Areas of Expertise
- Testosterone Replacement Therapy (TRT)
- Male Hypogonadism
- Endocrine Pharmacology
- Exercise Physiology
- Muscle Hypertrophy
- Sports Medicine
- Hormonal Health
- Evidence-Based Medical Writing
Medical Review
Medically Reviewed by Rebecca M. Collins, MD
Board-Certified Endocrinologist | Specialist in Men’s Hormonal Health
Dr. Rebecca M. Collins is a board-certified endocrinologist with extensive clinical experience in diagnosing and treating testosterone deficiency, pituitary disorders, metabolic diseases, osteoporosis, and endocrine conditions affecting adult men.
She reviews educational medical content to ensure consistency with current evidence-based clinical guidelines, focusing on diagnostic criteria, pharmacology, therapeutic indications, contraindications, laboratory monitoring, and long-term patient safety.
Medical Review Expertise
- Male Hypogonadism
- Testosterone Replacement Therapy
- Endocrine Disorders
- Bone Metabolism
- Hormonal Pharmacology
- Clinical Laboratory Interpretation
- Evidence-Based Medicine
Scientific Review
Scientific Review by Andrew P. Mitchell, PharmD, BCPS
Board-Certified Clinical Pharmacist | Specialist in Clinical Pharmacology
Dr. Andrew P. Mitchell is a board-certified clinical pharmacist whose expertise centers on endocrine pharmacotherapy, injectable hormone formulations, pharmacokinetics, drug safety, and therapeutic monitoring.
His scientific review process verifies the pharmacological accuracy of testosterone esters, dosing recommendations, absorption profiles, metabolism, adverse effect reporting, and consistency with FDA prescribing information, peer-reviewed clinical trials, and internationally recognized endocrine guidelines.
Scientific Review Expertise
- Clinical Pharmacology
- Testosterone Esters
- Pharmacokinetics
- Injectable Hormone Therapy
- Medication Safety
- Drug Monitoring
- Evidence-Based Pharmacotherapy
Related products
Trenon A 100mg/ml 10 ml (Trenbolone Acetate) – Medical Pharma
$103.00Read moreC20H24O3 = 312.4.
CAS — 10161-33-8 (Trenbolone); 10161-34-9 (Trenbolone Acetate).Pharmacopoeias
USP 31 (Trenbolone Acetate). Solution oily transparent color from light yellow to yellow, with characteristic odor. It should be stored at temperatures of 2° to 8°C for optimal storage conditions.
Trenon A contains: 100mg 100 mg / ml Trenbolone acetate.
Ultramix 300mg/ml 10 ml (Trenbolone Enanthate, Drostanolone Propionate, Testosterone Enanthate) – Medical Pharma
$103.00Read moreTrenbolone Enanthate
(17β)-3-Oxoestra-4,9,11-trien-17-yl heptanoate
C25H34O3 = 382.2
CAS — 10161-33-8Deposteron Testosterone Cypionate for sale 250mg/ml 10 ml M P Buy in USA
$93.00Read moreDeposteron
C27H40O3 = 412.6.
CAS — 58-20-8.
ATC — G03BA03.
ATC Vet — QG03BA03.USP 31(Testosterone Cypionate). A white or creamy-white, crystalline powder, odourless or has a slight odour. Insoluble in water; freely soluble in alcohol, in chloroform, in dioxan, and in ether; soluble in vegetable oils. Protect from light.
Testerone C contains: 250mg.
⦁ 250mg/ml Testosterone Cypionate.
Testosterone Online Purchase Enanthate 250mg/ml MP
$93.00Read moreC26H40O3 = 400.6.
CAS — 315-37-7.
ATC — G03BA03.
ATC Vet — QG03BA03.USP 31(Testosterone Enanthate). A white or creamy-white crystalline powder. It is odourless or has a faint odour characteristic of heptanoic acid. Insoluble in water; very soluble in ether; soluble in vegetable oils. Store at a temperature of 2°to 8°. Protect from light.
Testosterone E contains: 250mg 250 mg / ml Testosterone Enanthate.