Most Popular steroids USA
-
 Trenbolone 200 20ml - Sydgroup
$53.00
Trenbolone 200 20ml - Sydgroup
$53.00 -
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.
-
Somatrox XT Labs 150 IU x 10 vials (15 ui each)
Original price was: $450.00.$350.00Current price is: $350.00.













Sustanon 250mg/ml 10ml – Medical Pharma in USA
$95.00
Sustanon contains a mixture of four testosterone compounds, which were modified with the addition of carboxylic acid esters (propionic, propionic phenyl ester, isocaproic, and decanoic acids) at the 17-beta hydroxyl group.
Esterified forms of Testosterone are absorbed more slowly from the area of injection. Once in the bloodstream, the ester is removed to yield free (active) Testosterone.
Sustanon 250mg/ml 10ml – Medical Pharma Steroids Online in USA
Testosterone Decanoate
Decanoato de Testosterona; Testosteron Dekanoat; Testostérone, décanoate de; Testosteroni decanoas. 3-Oxoandrost-4-en-17β-yl Decanoate; 17β-Hydroxyandrost-4-en-3-one Decanoate.
C29H46O3 = 442.7.
CAS — 5721-91-5.
ATC — G03BA03.
ATC Vet — QG03BA03.
Pharmacopoeias. In Eur.(see p.vii).
Ph. Eur. 6.2(Testosterone Decanoate). A white or almost white powder. Practically insoluble in water; very soluble in anhydrous alcohol, in acetone, and in dichloromethane; freely soluble in fatty oils. Store at a temperature of 2°to 8°
Testosterone Isocaproate
Isocaproato de testosterona; Testosteron Isokaproat; Testostérone, isocaproate de; Testosterone Isohexanoate; Testosteroni isocaproas. 3-Oxoandrost-4-en-17β-yl 4-methylpentanoate; 17β-Hydroxyandrost-4-en-3-one 4-methylpentanoate.
C25H38O3 = 386.6.
CAS — 15262-86-9.
ATC — G03BA03.
ATC Vet — QG03BA03.
Pharmacopoeias. In Eur.(see p.vii).
Ph. Eur. 6.2(Testosterone Isocaproate). A white or almost white powder. Practically insoluble in water; very soluble in acetone and in dichloromethane; freely soluble in fatty oils.
Testosterone Phenylpropionate
Fenilpropionato de testosterona; Testosteron Fenilpropiyonat; Téstosterone, Phénylpropionate de; Testosteroni Phenylpropionas. 3-Oxoandrost-4-en-17β-yl 3-phenylpropionate; 17β-Hydroxyandrost-4-en-3-one 3-phenylpropionate.
C28H36O3 = 420.6.
CAS — 1255-49-8.
ATC — G03BA03.
ATC Vet — QG03BA03.
Pharmacopoeias. In BP(Vet).
BP(Vet) 2008(Testosterone Phenylpropionate). A white to almost white crystalline powder. Practically insoluble in water; sparingly soluble in alcohol. Protect from light.
Testosterone Propionate
NSC-9166; Propionato de testosterona; Testosteron Propiyonat; Testostérone, propionate de; Testosteroni propionas; Testosteronipropionaatti; Testosteronopropionatas; Testosteronpropionat; Testosteron-propionát; Testosteronu propionian; Tesztoszteronpropionát. 3-Oxoandrost-4-en-17β-yl propionate; 17β-Hydroxyandrost-4-en-3-one propionate.
C22H32O3 = 344.5.
CAS — 57-85-2.
ATC — G03BA03.
ATC Vet — QG03BA03.
Pharmacopoeias. In Chin., Eur.(see p.vii), Int., Jpn,and US.
Ph. Eur. 6.2(Testosterone Propionate). A white or almost white powder or colourless crystals. Practically insoluble in water; freely soluble in alcohol and in acetone; soluble in fatty oils.
USP 31(Testosterone Propionate). White or creamy-white, odourless, crystals or crystalline powder. Insoluble in water; freely soluble in alcohol, in dioxan, in ether, and in other organic solvents; soluble in vegetable oils. Protect from light.
Sustanon contains: 250mg
100mg/ml Testosterone Decanoate
60mg/ml Testosterone Isocaproate
60mg/ml Testosterone Phenylpropionate
30mg/mlTestosterone Propionate
Pharmacologic Category: Androgen
Dosing: Adult
250mg every three weeks; deep intramuscular injection.
Dosing: Geriatric
Refer to adult dosing.
Dosing: Pediatric
Safety and efficacy have not been adequately determined in children and adolescents. Pre-pubertal children treated with Sustanon should be treated with caution.
Dosing: Renal impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution due to propensity to cause edema.
Dosing: Hepatic impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution.
Use
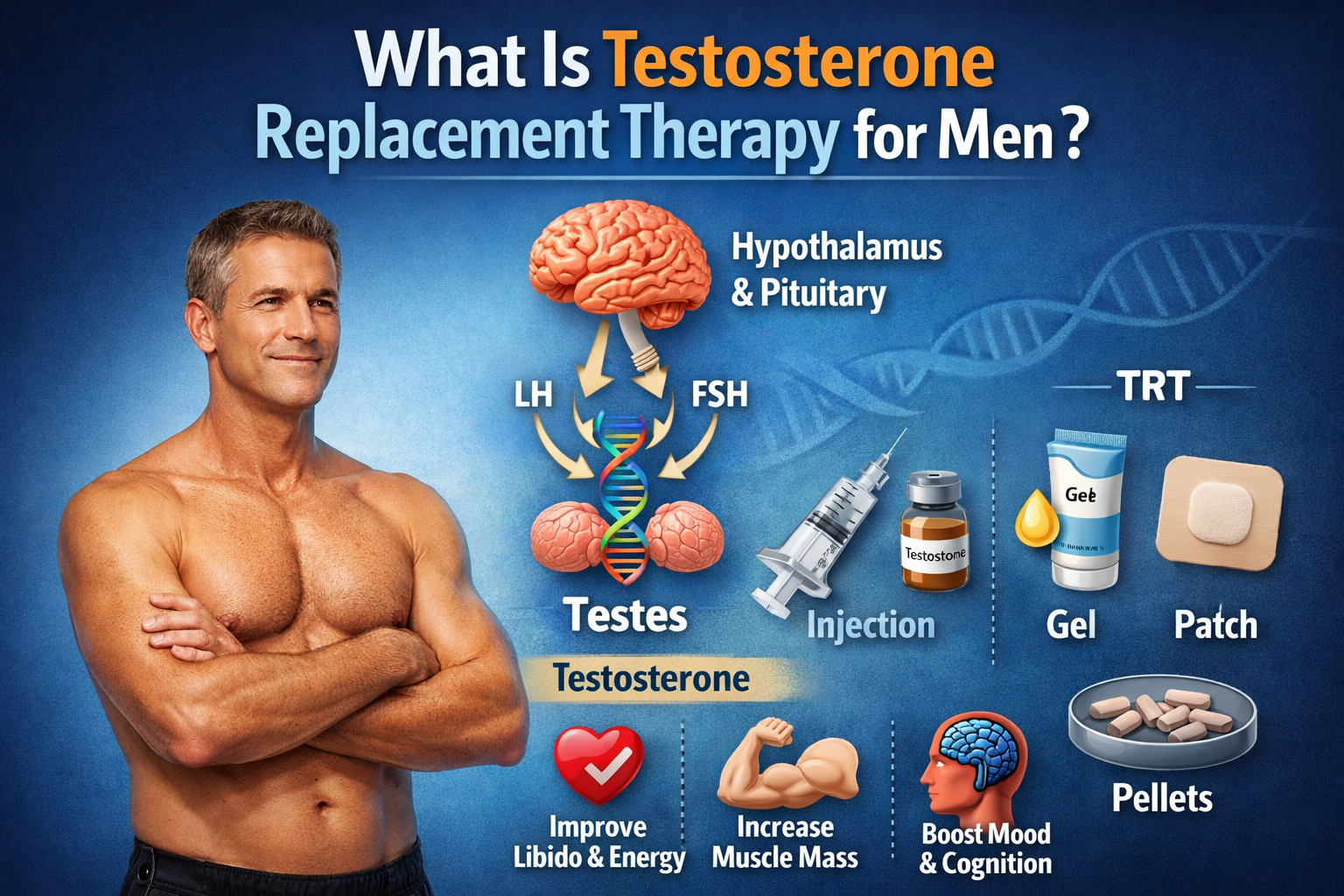
Testosterone replacement therapy for male hypogonadism, when testosterone deficiency has been confirmed by clinical features and biochemical tests.
Testosterone administration may also be used as supportive therapy for female-to-male transsexuals.
Storage/Stability
Store below 30°C.
Do not refrigerate or freeze.
Store in the original package in order to protect from light.
Contraindications
Pregnancy.
Known or suspected carcinoma of the prostate or breast.
Breast feeding.
Hypersensitivity to the active substance or to any of the excipients, including arachis oil. Sustanon is therefore contraindicated in patients allergic to peanuts or soya.
Warnings/Precautions
Medical examination:
Testosterone level should be monitored at baseline and at regular intervals during treatment. Clinicians should adjust the dosage individually to ensure maintenance of eugonadal testosterone levels.
Physicians should consider monitoring patients receiving Sustanon before the start of treatment, at quarterly intervals for the first 12 months and yearly thereafter for the following parameters:
Digital rectal examination (DRE) of the prostate and PSA to exclude benign prostate hyperplasia or a sub-clinical prostate cancer.
Haematocrit and haemoglobin to exclude polycythaemia.
In patients receiving long-term androgen therapy, the following laboratory parameters should also be monitored regularly: haemoglobin, and haematocrit, liver function tests and lipid profile.
Conditions that need supervision:
Patients, especially the elderly, with the following conditions should be monitored for:
Tumours – Mammary carcinoma, hypernephroma, bronchial carcinoma and skeletal metastases. In these patients hypercalcaemia or hypercalciuria may develop spontaneously, also during androgen therapy. The latter can be indicative of a positive tumour response to the hormonal treatment. Nevertheless, the hypercalcaemia or hypercalciuria should first be treated appropriately and after restoration of normal calcium levels, hormone therapy can be resumed.
Pre-existing conditions
In patients suffering from severe cardiac, hepatic or renal insufficiency or ischaemic heart disease, treatment with testosterone may cause severe complications characterised by oedema with or without congestive cardiac failure. In such cases treatment must be stopped immediately. Patients who experienced myocardial infarction, cardiac-, hepatic- or renal insufficiency, hypertension, epilepsy, or migraine should be monitored due to the risk of deterioration of or reoccurrence of disease. In such cases treatment must be stopped immediately.
Testosterone may cause a rise in blood pressure and Sustanon 250 should be used with caution in men with hypertension.
Epilepsy or Migraine – (or a history of these conditions), since androgens may occasionally induce fluid and sodium retention.
Diabetes mellitus – Androgens in general and Sustanon can improve glucose tolerance in diabetic patients.
Anti-coagulant therapy – Androgens in general and Sustanon can enhance the anti-coagulant action of coumarin-type agents.
Sleep apnea- Caution should be applied when treating men with sleep apnea. There have been reports that testosterone can cause or exacerbate pre-existing sleep apnea. However, there is a lack of evidence regarding the safety of testosterone in men with the condition. Good clinical judgment and caution should be employed in patients with risk factors such as adiposity or chronic lung diseases.
Pregnancy risk factor X
Category X: Studies in animals or human beings have demonstrated fetal abnormalities, or there is evidence of fetal risk based on human experience, or both, and the risk of the use of the drug in pregnant women clearly outweighs any possible benefit. The drug is contraindicated in women who are or may become pregnant.
Pregnancy considerations
Use is contraindicated in women who are or may become pregnant; masculinization of the fetus has been reported.
Lactation
Excreted in breast milk.
Breast feeding considerations
Sustanon is excreted in breast milk. Due to the potential for serious adverse reactions in the nursing infant, breast-feeding is not recommended.
Adverse reactions
Frequency unknown.
Cardiovascular: Edema.
Central nervous system: Depression, excitation, insomnia.
Dermatologic: Acne (females and prepubertal males).
Also reported in females: Hirsutism, male-pattern baldness.
Endocrine & metabolic: Electrolyte imbalances, glucose intolerance, gonadotropin secretion inhibited, gynecomastia, HDL decreased, LDL increased, libido changes.
Also reported in females: Clitoral enlargement, menstrual irregularities.
Genitourinary:
Prepubertal males: Increased or persistent erections, penile enlargement.
Postpubertal males: Bladder irritation, epididymitis, impotence, oligospermia, priapism (chronic), testicular atrophy, testicular function inhibited.
Hematologic: Prothrombin time increased, suppression of clotting factors.
Hepatic: Alkaline phosphatase increased, ALT increased, AST increased, bilirubin increased, cholestatic jaundice, hepatic necrosis (rare), hepatocellular neoplasms, peliosis hepatis (with long-term therapy)
Neuromuscular & skeletal: CPK increased, premature closure of epiphyses (in children).
Renal: Creatinine excretion increased.
Drug interactions
Enzyme-inducing agents may decrease and enzyme-inhibiting drugs may increase testosterone levels. Therefore, adjustment of the dose of Sustanon may be required.
Insulin and other anti-diabetic medicines:
Androgens may improve glucose tolerance and decrease the need for insulin or other anti-diabetic medicines in diabetic patients.
Patients with diabetes mellitus should therefore be monitored especially at the beginning or end of treatment and at periodic intervals during Sustanon treatment.
Anti-coagulant therapy:
High doses of androgens may enhance the anticoagulant action of coumarin type agents. Therefore, close monitoring of prothrombin time and if necessary a dose reduction of the anti-coagulant is required during therapy.
ACTH or corticosteroids:
The concurrent administration of testosterone with ACTH or corticosteroids may enhance oedema formation therefore these active substances should be administered cautiously, particularly in patients with cardiac or hepatic disease or in patients predisposed to edema.
Test interactions
Androgens may decrease levels of thyroxine-binding globulin, resulting in decreased total T4 serum levels and increased resin uptake of T3 and T4. Free thyroid hormone levels remain unchanged, and there is no clinical evidence of thyroid dysfunction.
Monitoring parameters
Liver function tests, cholesterol profile, hemoglobin/hematocrit; INR/PT in patients on anticoagulant therapy.
Children: Radiographs of left wrist and hand every 6 months (to assess bone maturation).
Adult females: Signs of virilization (deepening voice, hirsutism, acne, clitoromegaly); urine and serum calcium in women with breast cancer.
Dosage forms
Glass ampules; 1ml
Anatomic Therapeutic Chemical (ATC) Classification
ATC — G03BA03.
Mechanism of action
Testosterone is the principal endogenous androgen responsible for promoting the growth and development of the male sex organs and maintaining secondary sex characteristics in androgen-deficient males. It has anabolic properties over skeletal muscle that increase with the dosing.
Pharmacodynamics/Kinetics
Sustanon contains four esters of testosterone with different durations of action. The esters are hydrolysed into the natural hormone testosterone as soon as they enter the general circulation.
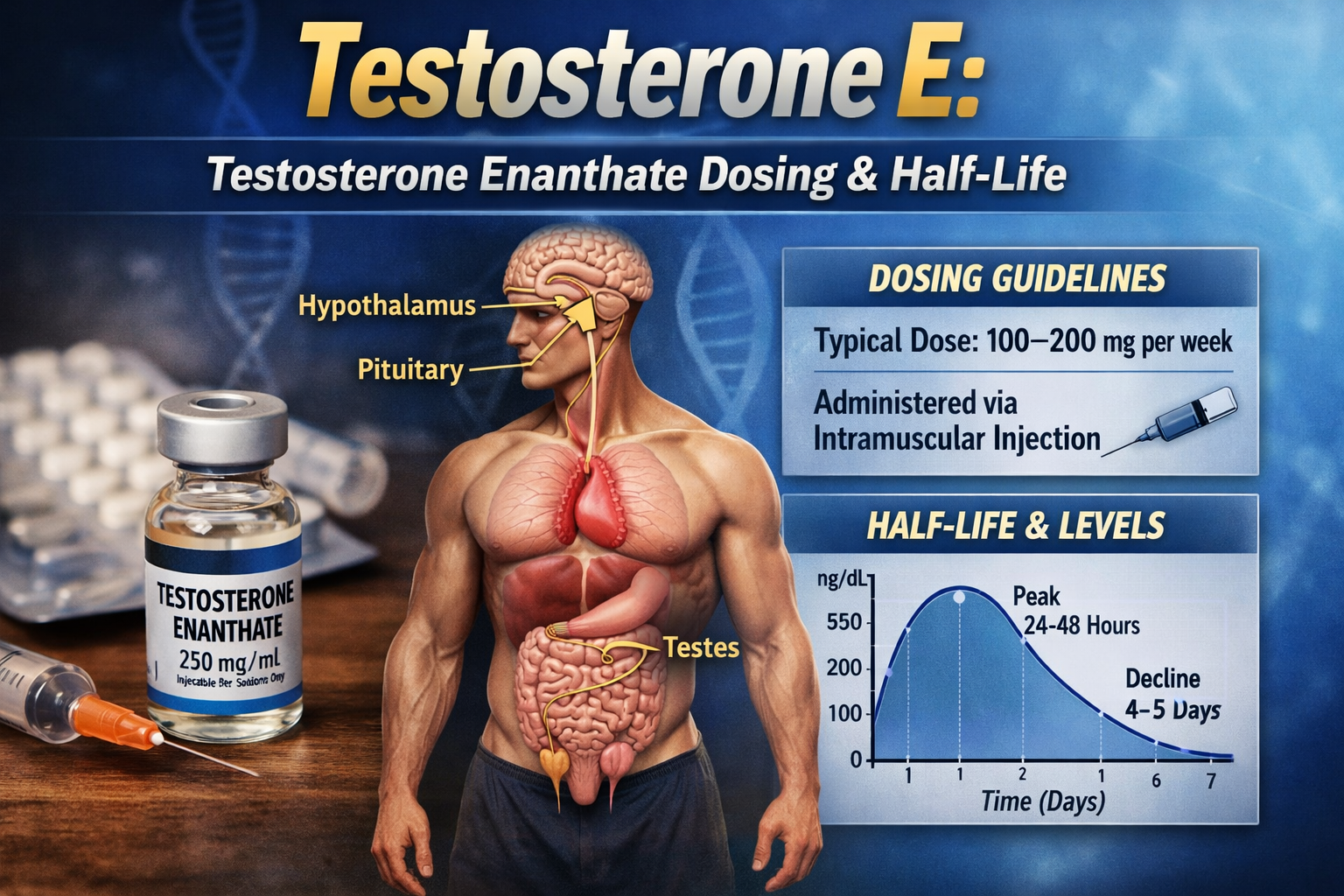
Absorption:
A single dose of Sustanon leads to an increase of total plasma testosterone with peak levels of approximately 70nmol/l (Cmax), which are reached approximately 24-48 h (tmax) after administration. Plasma testosterone levels return to the lower limit of the normal range in males in approximately 21 days.
In female-to-male transsexuals, a single dose of Sustanon repeated every two weeks resulted in mean trough testosterone levels towards the upper end of the normal male range at 2, 4 and 12 months.
Distribution:
Testosterone displays a high (over 97%) non-specific binding to plasma proteins and sex hormone binding globulin in in vitro tests.
Biotransformation:
Testosterone is metabolised to dihydrotestosterone and estradiol, which are further metabolised via the normal pathways.
Elimination:
Excretion mainly takes place via the urine as conjugates of etiocholanolone and androsterone.
Buy Testosterone steroids online USA.
Related products
Provir (Mesterolone) 50mg/tab 100 tabs – Medical Pharma
$93.00Read morePharmacologic Category
Androgen.
Dosing: Adult
50mg every days for duration of 4-8 weeks.
Dosing: Geriatric
Refer to adult dosing.
Dosing: Pediatric
No information in pediatric population available.
Dosing: Renal impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution due to propensity to cause edema.
Dosing: Hepatic impairment
No dosage adjustment provided in manufacturer’s labeling; use with caution.
Primobolan 100mg/ml 10ml – Medical Pharma Anabolic Steroids USA
$103.00Add to cartMetenolone Enantate; Enantato de metenolona; Enantato de Metilandrostenolona;
Méténolone, Enantate de; Metenoloni Enantas; Methenolone; Enanthate (USAN); Methenolone Oenanthate; NSC-64967; SH-601; SQ-16374. 17β-Hydroxy-1-methyl-5α-androst-1-en-3-one-heptanoate.
Megabol 200mg/ml 10ml – Medical Pharma
$99.00Add to cartMetandienone (pINN); Metandienon; Metandienona; Métandiénone; Metandienoni; Metandienonum; Methandrostenolone; NSC-42722.17β-Hydroxy-17α-methylandrosta-1,4 dien-3-one.
C20H28O2 = 300.4.
CAS — 72-63-9.
ATC — A14AA03; D11AE01.
ATC Vet — QA14AA03; QD11AE01.NSC-9166; Propionato de testosterona; Testosteron Propiyonat; Testostérone, propionate de; Testosteroni propionas; Testosteronipropionaatti; Testosteronopropionatas; Testosteronpropionat; Testosteron-propionát; Testosteronu propionian; Tesztoszteronpropionát. 3-Oxoandrost-4-en-17β-yl propionate; 17β-Hydroxyandrost-4-en-3-one propionate.
Mastabol 100mg/ml 10ml – Medical Pharma Buy in USA
$93.00Add to cartMastabol 100mg/ml (10ml) by Medical Pharma is a premium Drostanolone Propionate formula designed to enhance muscle hardness, strength, and fat loss. Ideal for cutting cycles, it promotes a lean, defined physique while maintaining high performance. Available for secure purchase in the USA with fast shipping and a trusted buying process.