Most Popular steroids USA
-
 Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00 -
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.
-
Somatrox XT Labs 150 IU x 10 vials (15 ui each)
Original price was: $450.00.$350.00Current price is: $350.00.











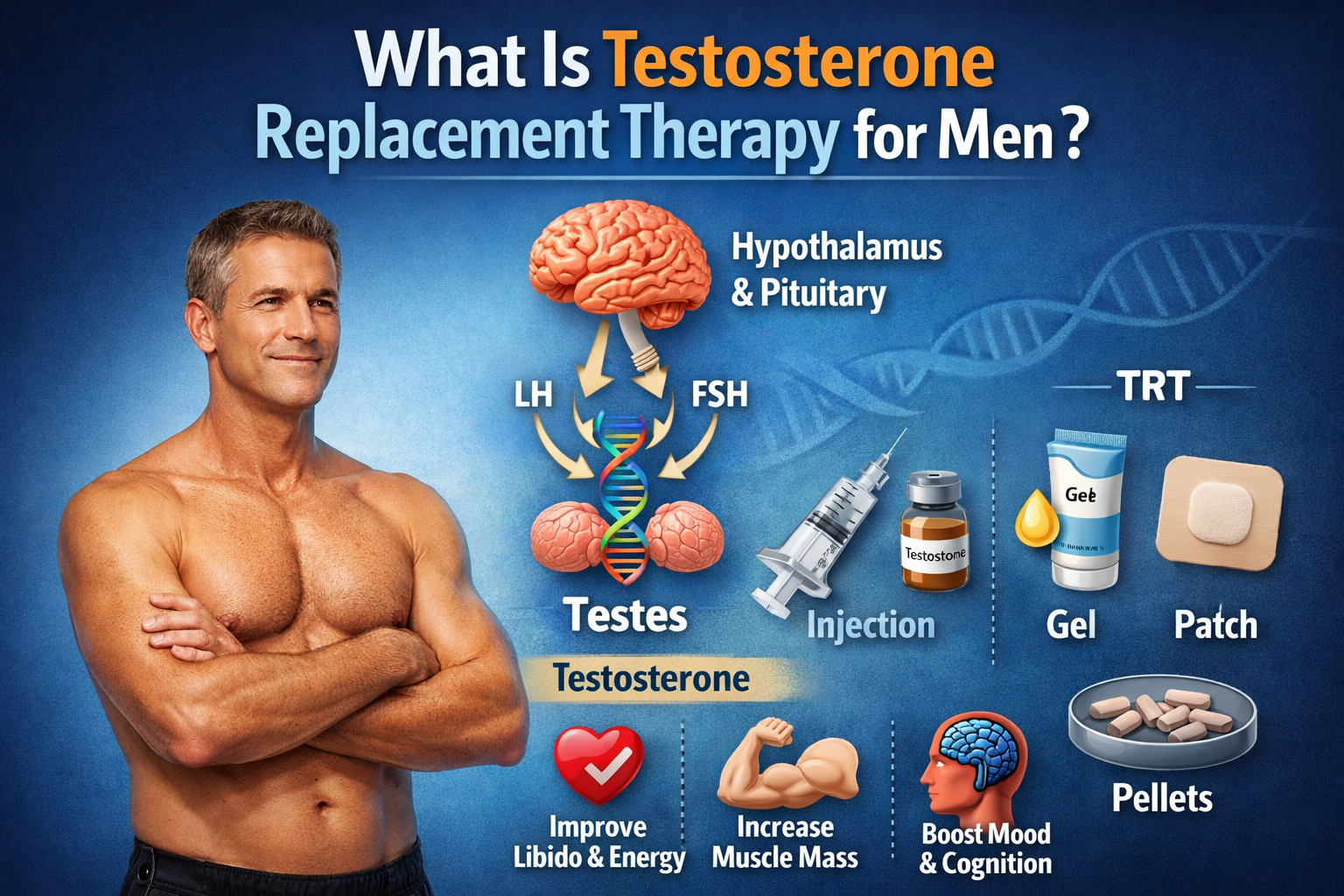
What is testosterone replacement therapy for men? Testosterone replacement therapy (TRT) supplements or replaces testosterone to treat male hypogonadism and bring levels into the mid-normal range. Low testosterone disrupts the hypothalamic-pituitary-gonadal axis and can reduce libido, muscle mass, bone density and red blood cell production. Men with persistent symptoms such as low libido, fatigue or loss of muscle should understand how testosterone replacement therapy works, its risks and benefits, and how low testosterone is diagnosed before deciding on treatment.
Common formulations include short- and long-ester intramuscular or subcutaneous injections, transdermal gels and patches, and subdermal pellet implants. Injections often produce peaks and troughs depending on dosing cadence, gels and patches provide steadier daily levels, and pellets release hormone over months. Choice of ester and dosing schedule affects symptom fluctuation and the optimal timing for laboratory tests. Diagnosis requires characteristic symptoms plus consistently low morning serum testosterone on at least two separate tests, with a typical total testosterone cutoff near 300 ng/dL(5); measuring luteinizing hormone helps distinguish primary from secondary hypogonadism and guides further evaluation when results are low or inconsistent.
Key takeaways
- TRT supplements or replaces deficient testosterone to relieve hypogonadal symptoms and restore mid-normal levels; it aims to improve function while keeping levels within a physiologic range.
- Treatment is appropriate when characteristic symptoms coincide with consistently low morning testosterone on two tests; measuring luteinizing hormone helps classify primary versus secondary causes.
- Injections, gels, patches and pellets differ in convenience, cost and blood-level stability; choose a formulation based on symptom control, monitoring needs and lifestyle.
- Most men see reliable improvements in libido, modest gains in erectile function and increases in lean mass and energy when dosing is appropriate; those with the lowest baseline levels tend to benefit most.
- Baseline labs and ongoing monitoring, including hematocrit, PSA and testosterone, help manage risks such as erythrocytosis and prostate changes; regular follow-up allows dose adjustments or therapy pauses when needed.
How testosterone replacement therapy works
TRT treats confirmed testosterone deficiency by restoring physiologic androgen levels to reduce hypogonadal symptoms(1). The hypothalamus signals the pituitary to release luteinizing hormone, and luteinizing hormone stimulates the testes to produce testosterone; when any part of this axis is impaired, blood testosterone falls and symptoms appear. Testosterone supports sexual function, muscle and bone health, and red blood cell production, so restoring levels aims to normalize those systems while balancing safety monitoring and individual goals.
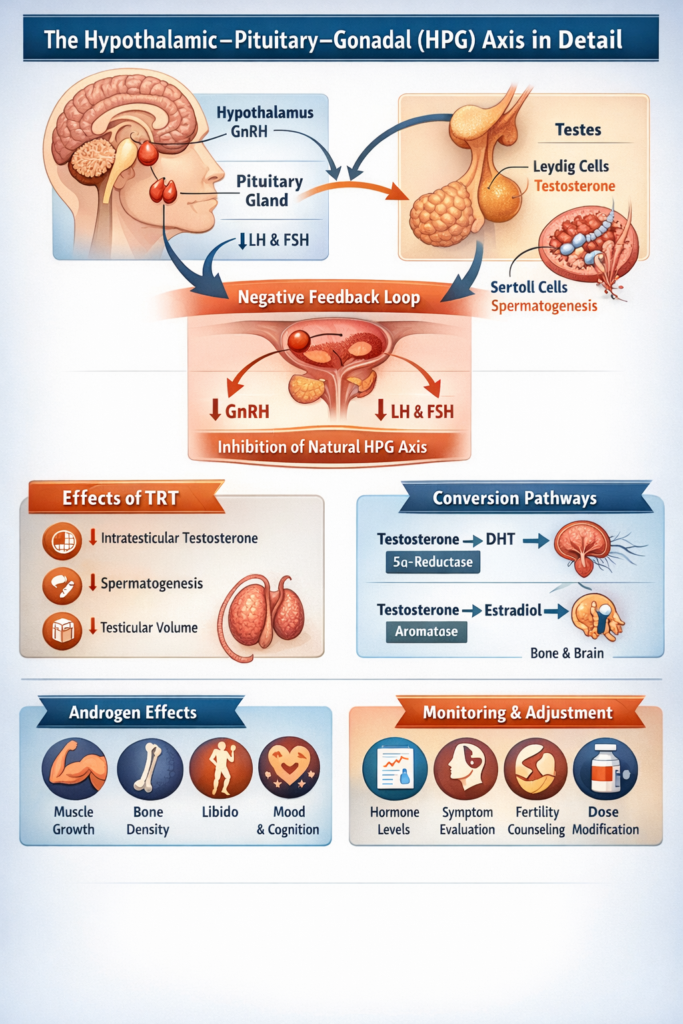
The hypothalamic–pituitary–gonadal (HPG) axis in detail
The HPG axis operates through tightly regulated negative feedback. Gonadotropin-releasing hormone (GnRH) is secreted in a pulsatile manner by the hypothalamus, stimulating the anterior pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH acts on Leydig cells in the testes to produce testosterone, while FSH supports Sertoli cell function and spermatogenesis.
Circulating testosterone and its metabolites—particularly estradiol—provide negative feedback at both the hypothalamic and pituitary levels. Even small disruptions in this feedback loop can significantly alter circulating androgen levels.
When TRT is introduced, exogenous testosterone bypasses hypothalamic and pituitary control. This suppresses endogenous GnRH, LH and FSH secretion through feedback inhibition. As a result:
- Intratesticular testosterone declines.
- Spermatogenesis decreases.
- Testicular volume may reduce over time.
Understanding this suppression is central to patient counseling, particularly in men concerned about fertility.
Serum testosterone versus tissue-level androgen activity
Testosterone exerts its biological effects by binding to intracellular androgen receptors (AR). Once activated, the androgen receptor complex translocates to the nucleus and influences gene transcription involved in:
- Muscle protein synthesis
- Erythropoiesis
- Bone remodeling
- Libido and sexual signaling pathways
- Mood and neurocognitive modulation
However, circulating total testosterone does not always perfectly reflect tissue androgen activity. Factors that influence bioavailability include:
- Sex hormone-binding globulin (SHBG) levels
- Albumin binding
- Local enzyme activity in tissues
In men with abnormal SHBG levels (e.g., obesity, hyperthyroidism, liver disease), free testosterone may better correlate with symptoms than total testosterone alone.
TRT aims to restore serum levels to a physiologic mid-normal range, but clinical response—not just laboratory value—guides dose optimization.
Conversion pathways: DHT and estradiol
Testosterone is not the final active molecule in many tissues. It undergoes enzymatic conversion:
5-alpha reduction to dihydrotestosterone (DHT)
In tissues such as prostate, skin and hair follicles, testosterone converts to DHT via 5-alpha reductase. DHT binds the androgen receptor with greater affinity and drives:
- Prostate growth
- Facial and body hair development
- Scalp hair miniaturization in predisposed men
TRT may increase DHT levels proportionally, depending on dose and individual enzymatic activity.
Aromatization to estradiol
Testosterone is also converted to estradiol by the aromatase enzyme, especially in adipose tissue. Estradiol plays critical roles in:
- Bone mineral density maintenance
- Libido modulation
- Vascular function
- Central nervous system regulation
Complete suppression of estradiol is undesirable. Balanced aromatization is physiologically necessary for optimal outcomes.
Pharmacokinetics: how delivery method influences physiology
Different TRT formulations produce distinct serum concentration curves:
- Short-ester injections may create peak-and-trough fluctuations.
- More frequent subcutaneous dosing tends to smooth hormonal variability.
- Transdermal preparations provide steadier daily exposure.
- Pellets release hormone slowly over months but are less adjustable.
These pharmacokinetic differences can influence:
- Mood stability
- Libido consistency
- Hematocrit rise
- Estradiol conversion
- Symptom fluctuation between doses
The goal is not supraphysiologic exposure but stable androgen signaling within a normal biologic range.
Time course of physiologic response
TRT does not produce uniform effects simultaneously. Clinical improvements follow a predictable biological timeline:
- Libido: often improves within 2–4 weeks.
- Erectile function: may improve within 1–3 months.
- Lean mass increases: typically noticeable after 8–12 weeks.
- Strength gains: develop progressively with resistance training.
- Bone density improvements: accumulate over 12–24 months.
- Hematocrit elevation: may appear within 3–6 months.
Understanding this timeline helps align patient expectations with biological reality.
Functional versus organic hypogonadism
TRT may be considered in different pathophysiologic contexts:
Primary hypogonadism (testicular failure)
- Elevated LH
- Low testosterone
- Often irreversible
- Typically strong response to TRT
Secondary hypogonadism (pituitary or hypothalamic dysfunction)
- Low or inappropriately normal LH
- May require further endocrine evaluation
- Some cases are reversible
Functional suppression
Common in:
- Obesity
- Chronic illness
- Severe stress
- Sleep deprivation
In these cases, lifestyle optimization may partially restore endogenous production, and TRT should be considered carefully.
Restoring physiologic signaling, not “boosting” hormones
The objective of TRT is not enhancement beyond normal human physiology. It is restoration of androgen signaling to a range that supports:
- Metabolic stability
- Sexual health
- Musculoskeletal integrity
- Hematologic balance
Dose titration aims to achieve symptom resolution while minimizing:
- Erythrocytosis
- Excess estradiol symptoms
- Suppression-related fertility concerns
The therapy must be individualized, monitored and adjusted over time rather than treated as a fixed-dose intervention.
Who qualifies for testosterone replacement therapy for men
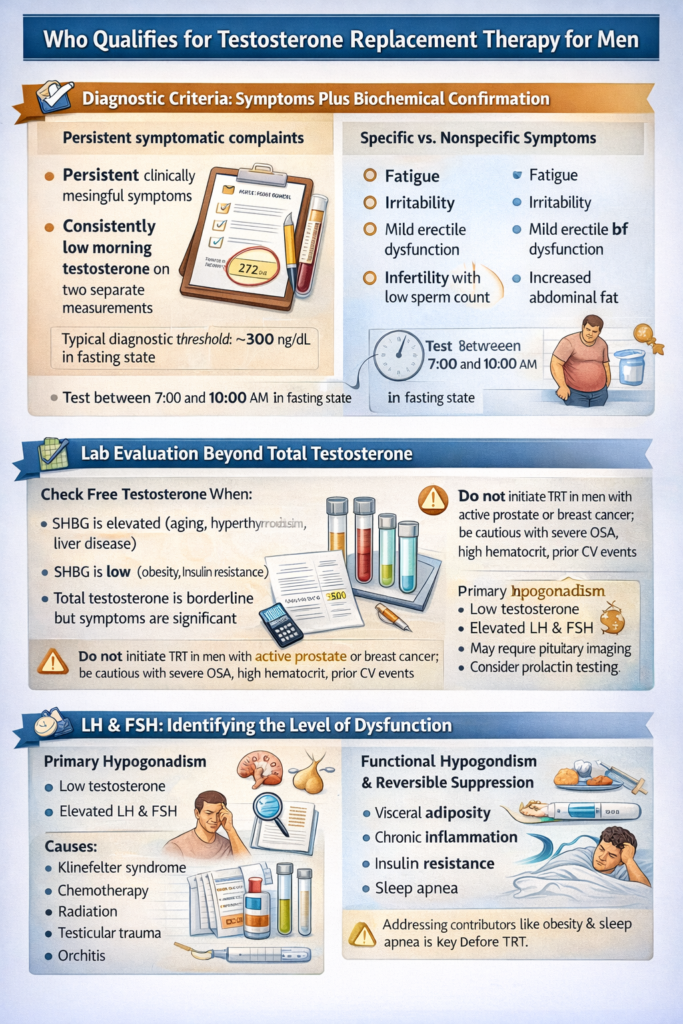
Clinicians consider TRT only when characteristic signs and symptoms are present and laboratory testing confirms low testosterone. Be specific about onset, severity and whether symptoms are progressive, because many complaints such as fatigue or low libido are nonspecific. Highly specific findings such as loss of facial or body hair and very small testicular volume strongly suggest hypogonadism and should prompt focused evaluation.
Common clinical features include low libido or decreased sexual desire, erectile dysfunction or fewer morning erections, depressed mood or persistent fatigue, decreased muscle mass with increased central fat, and reduced body or facial hair with small testicles. Documenting these findings on history and physical exam helps separate true hypogonadism from other causes and guides testing.
Measure free testosterone or calculate it when total T is borderline or sex hormone-binding globulin (SHBG) is abnormal, and check LH and FSH to determine primary versus secondary causes; low or inappropriately normal LH suggests pituitary evaluation and possible endocrinology referral. Absolute contraindications include active prostate or breast cancer, while relative concerns include hematocrit greater than 50 percent, untreated severe obstructive sleep apnea, and recent major cardiovascular events. Men who want to preserve fertility should discuss sperm-sparing options such as human chorionic gonadotropin or selective estrogen receptor modulators and seek reproductive or urology referral before starting therapy.
Diagnostic criteria: symptoms plus biochemical confirmation
TRT is not indicated for laboratory values alone. Diagnosis requires:
- Persistent, clinically meaningful symptoms.
- Consistently low morning testosterone on at least two separate measurements.
Testing should be performed:
- Between 7:00 and 10:00 AM.
- In a fasting state when possible.
- Without acute illness or recent major stressors.
A typical diagnostic threshold for total testosterone is near 300 ng/dL, but clinical context matters. Men with borderline levels (e.g., 280–350 ng/dL) and significant symptoms may require further evaluation rather than automatic exclusion.
Laboratory confirmation is the foundation; symptom correlation determines clinical relevance.
Distinguishing specific from nonspecific symptoms
Many symptoms attributed to “low T” overlap with common conditions such as depression, sleep deprivation, metabolic syndrome and chronic stress.
Highly specific findings
These increase the likelihood of true hypogonadism:
- Loss of spontaneous morning erections
- Decreased shaving frequency
- Reduced testicular volume (< 15 mL)
- Infertility with low sperm count
- Delayed puberty (in younger men)
Nonspecific findings
These require careful differential diagnosis:
- Fatigue
- Irritability
- Mild erectile dysfunction
- Increased abdominal fat
- Reduced motivation
The more specific the symptom cluster, the stronger the diagnostic suspicion.
Laboratory evaluation beyond total testosterone
Total testosterone alone may be misleading in certain physiologic states.
When to measure free testosterone
Free testosterone should be measured or calculated when:
- SHBG is elevated (aging, hyperthyroidism, liver disease).
- SHBG is low (obesity, insulin resistance, nephrotic syndrome).
- Total testosterone is borderline but symptoms are significant.
Calculated free testosterone using equilibrium dialysis–validated formulas is often more clinically useful than direct analog assays.
LH and FSH: identifying the level of dysfunction
Gonadotropin levels clarify etiology.
Primary hypogonadism (testicular failure)
- Low testosterone
- Elevated LH and FSH
- Often irreversible
- Strong indication for TRT
Causes may include:
- Klinefelter syndrome
- Chemotherapy
- Radiation
- Testicular trauma
- Orchitis
Secondary hypogonadism (hypothalamic or pituitary)
- Low testosterone
- Low or inappropriately normal LH
- May require pituitary imaging
- Consider prolactin testing
Potential causes include:
- Pituitary adenoma
- Chronic opioid use
- Severe obesity
- Hyperprolactinemia
- Chronic systemic illness
Identifying secondary causes is critical before initiating therapy.
Functional hypogonadism and reversible suppression
In many men, especially those with obesity or metabolic syndrome, low testosterone reflects reversible suppression rather than permanent gland failure.
Contributing factors include:
- Visceral adiposity (increased aromatization)
- Chronic inflammation
- Insulin resistance
- Sleep apnea
- Psychological stress
In these cases, weight loss, improved sleep and metabolic correction may partially restore endogenous production. TRT should not replace lifestyle intervention when reversible contributors are present.
Absolute contraindications
TRT should not be initiated in men with:
- Active prostate cancer
- Active male breast cancer
- Known hypersensitivity to testosterone formulations
These conditions require specialized management.
Relative contraindications and caution zones
Certain conditions require stabilization or careful monitoring before starting therapy:
- Hematocrit > 50%
- Untreated severe obstructive sleep apnea
- Recent myocardial infarction or stroke
- Severe lower urinary tract symptoms
- Thrombophilia or prior thromboembolic events
In these cases, risk–benefit discussion and specialist input are often appropriate.
Fertility considerations and suppression of spermatogenesis
Exogenous testosterone suppresses intratesticular testosterone production, which is required for sperm generation(1)(5). Even men with normal baseline fertility may experience:
- Reduced sperm concentration
- Oligospermia
- Azoospermia
Men who wish to preserve fertility should consider alternatives such as:
- Human chorionic gonadotropin (hCG) to stimulate Leydig cells
- Selective estrogen receptor modulators (e.g., clomiphene)
- Combination approaches under specialist care
Fertility planning should occur before starting TRT, not after suppression has occurred.
Age-related decline versus pathologic hypogonadism
Age-related testosterone decline alone does not automatically justify TRT.
Key distinctions:
- Physiologic aging involves gradual decline.
- Pathologic hypogonadism involves symptomatic androgen deficiency with confirmed low levels.
Treatment decisions should prioritize symptom burden and biochemical confirmation rather than age alone.
Clinical decision-making framework
A simplified qualification algorithm:
- Assess symptoms.
- Confirm low morning testosterone twice.
- Evaluate SHBG and free testosterone if borderline.
- Measure LH/FSH to classify etiology.
- Rule out contraindications.
- Discuss fertility goals.
- Individualize therapy plan.
Only after completing this sequence should TRT be initiated.
Evidence-based benefits men can expect from TRT
Randomized trials and meta-analyses show consistent sexual benefits for men with low baseline testosterone (2). Most experience increased libido and modest improvements in erectile function, with early changes appearing within weeks and further gains over several months. Effect sizes for sexual desire and erectile outcomes are generally small to moderate, and men with the lowest starting levels tend to benefit most.
Clinical trials also demonstrate increases in lean body mass, reductions in fat mass and measurable gains in bone mineral density, particularly at the lumbar spine. Muscle and strength gains usually develop over months and bone benefits accumulate over a year or more, and combining TRT with progressive resistance training and adequate protein intake increases the likelihood of meaningful improvement. Improvements in mood, energy and cognitive performance are less predictable, so treat mood disorders separately when present and set realistic expectations about nonsexual benefits. Some specific work on topical formulations and mood shows potential benefits in men with depression; see findings on testosterone gel supplementation for men with depression for more context.
Below are the key risks and monitoring triggers to weigh against potential benefits. Understanding these issues helps patients and clinicians choose an approach that balances benefits, safety and individual goals.
Sexual function: the most consistently demonstrated benefit
Sexual symptoms are the domain where TRT shows the strongest and most reproducible effects.
Libido and sexual desire
Randomized controlled trials consistently demonstrate:
- Moderate improvement in sexual desire
- Increased sexual thoughts and initiation
- Improved overall sexual satisfaction
Men with:
- Total testosterone well below 250 ng/dL
- Clear baseline sexual dysfunction
tend to experience the largest relative improvement.
Libido often improves within 2–4 weeks, making it one of the earliest markers of therapeutic response.
Erectile function
Erectile function improvements are typically:
- Modest rather than dramatic
- More pronounced in men with true hypogonadism
TRT is not a direct vasodilator like PDE5 inhibitors. Instead, it enhances:
- Nitric oxide synthase activity
- Penile tissue androgen receptor signaling
- Responsiveness to PDE5 inhibitors
In men with borderline erectile dysfunction and low testosterone, TRT may improve PDE5 inhibitor responsiveness.
However, severe vasculogenic erectile dysfunction often requires additional therapy.
Body composition: lean mass and fat redistribution
TRT produces measurable changes in body composition.
Lean body mass
Most trials demonstrate:
- Increases in lean mass within 8–12 weeks
- Progressive gains over 6–12 months
Mechanisms include:
- Increased muscle protein synthesis
- Satellite cell activation
- Enhanced neuromuscular efficiency
- Reduced myostatin signaling
Strength improvements correlate strongly with concurrent resistance training.
Without exercise stimulus, gains are smaller but still measurable.
Fat mass reduction
Testosterone improves body composition by:
- Reducing visceral adiposity
- Improving insulin sensitivity
- Decreasing fat mass percentage
The effect size is moderate and typically develops gradually over months.
Men with metabolic syndrome often experience both hormonal and metabolic improvements.
Bone mineral density: long-term structural benefit
Testosterone plays a central role in bone metabolism.
Benefits include:
- Increased lumbar spine bone mineral density
- Slower progression of osteopenia
- Reduced fracture risk in long-term observational data
Estradiol conversion is critical here. Adequate aromatization supports:
- Osteoblast activity
- Bone remodeling balance
Bone density improvements typically require 12–24 months to become measurable.
Hematologic effects: erythropoiesis and oxygen capacity
Testosterone stimulates erythropoietin production and red blood cell formation.
Clinical effects include:
- Increased hemoglobin
- Increased hematocrit
- Improved anemia in hypogonadal men
This may improve exercise tolerance and perceived energy in men with baseline anemia.
However, excessive erythrocytosis is a dose-dependent risk requiring monitoring.
Mood, cognition and psychological effects(2)
Evidence in this domain is mixed.
Some trials show:
- Mild improvements in depressive symptoms
- Increased motivation
- Enhanced sense of well-being
Effects appear strongest in:
- Men with clinically low testosterone
- Men with mild depressive symptoms rather than major depressive disorder
Cognitive improvements (memory, executive function) are inconsistent across studies.
TRT should not replace psychiatric treatment when primary mood disorders are present.
Metabolic and cardiometabolic markers
Emerging evidence suggests TRT may improve:
- Insulin sensitivity
- Waist circumference
- Fasting glucose in hypogonadal men with metabolic syndrome
- Lipid parameters (variable effect)
However, these changes are generally modest and should complement—not replace—dietary and lifestyle intervention.
Time course of expected benefits
Different physiologic systems respond at different speeds.
| Effect | Approximate Onset | Stabilization |
|---|---|---|
| Libido | 2–4 weeks | 3 months |
| Erectile response | 1–3 months | 6 months |
| Lean mass | 8–12 weeks | 6–12 months |
| Fat reduction | 3–6 months | Ongoing |
| Bone density | 6–12 months | 24+ months |
| Hemoglobin increase | 3 months | 6–12 months |
Understanding this timeline prevents premature dose escalation.
Dose–response relationship
More is not necessarily better.
Supraphysiologic dosing may:
- Increase erythrocytosis risk
- Elevate estradiol excessively
- Worsen lipid profiles
- Increase adverse effects
Most benefits occur when serum testosterone is restored to mid-normal physiologic range rather than high-normal or supraphysiologic levels.
Who benefits the most?
Evidence consistently shows stronger response in:
- Men with clearly low baseline testosterone
- Men with pronounced sexual symptoms
- Men without severe vascular comorbidities
- Men who combine therapy with resistance training
Men with borderline levels and nonspecific symptoms may experience smaller or inconsistent benefit.
Realistic expectations: restoration, not enhancement
TRT restores deficient androgen signaling. It does not:
- Create supranormal athletic performance
- Reverse decades of sedentary lifestyle
- Cure primary mood disorders
- Replace cardiovascular risk management
Patients with appropriate expectations report higher satisfaction and better long-term adherence.
Risks, side effects and monitoring triggers
Testosterone increases red blood cell mass(1)(5), so hematocrit monitoring is essential. Obtain a baseline complete blood count, recheck at three to six months after starting therapy and then at least annually. Many clinicians act before hematocrit reaches 54 percent, with thresholds such as 50 percent prompting dose reduction, temporary cessation or therapeutic phlebotomy until values fall; investigate other causes of erythrocytosis when appropriate.
Cardiovascular safety is complex and findings differ by study design and population(6)(8)(9). Some large trials in selected hypogonadal men did not show a clear increase in major adverse cardiac events, while observational studies and pooled analyses have reported signals for thrombotic and other events. Professional summaries like the ACC summary on cardiovascular safety discuss this nuanced evidence. Regulatory bodies have also issued guidance; for example, the FDA cautions about testosterone products emphasize careful diagnosis and monitoring.
Monitor prostate health with a baseline digital rectal exam and PSA, then repeat PSA periodically; refer to urology for abnormal values such as PSA above 4.0 ng/mL or a rise greater than 1.4 ng/mL within 12 months. Counsel men that TRT suppresses spermatogenesis and can reduce testicular volume, and recommend semen evaluation and sperm-sparing strategies for those planning fertility. Discussing these issues before starting therapy helps avoid preventable complications and ensures timely referral when needed.
Erythrocytosis: the most common dose-dependent adverse effect
Testosterone stimulates erythropoiesis through:
- Increased erythropoietin production
- Direct bone marrow stimulation
- Suppression of hepcidin (increasing iron availability)
This can lead to elevated hemoglobin and hematocrit.
Why it matters
Elevated hematocrit increases blood viscosity, which may:
- Increase thrombotic risk
- Worsen hypertension
- Increase stroke risk in predisposed individuals
Risk appears higher with:
- Injectable formulations (especially higher peaks)
- Supraphysiologic dosing
- Older age
- Sleep apnea
Monitoring strategy
- Baseline CBC
- Repeat at 3–6 months
- Then annually (or more frequently if trending upward)
Clinical action thresholds:
- ≥50%: consider dose adjustment
- ≥52–54%: reduce dose, pause therapy, or initiate therapeutic phlebotomy
Persistent elevation warrants evaluation for:
- Undiagnosed sleep apnea
- Smoking
- Dehydration
- Underlying myeloproliferative disorders
Cardiovascular risk: signal versus causation
The cardiovascular debate surrounding TRT is nuanced.
Mechanistic considerations
Testosterone may:
- Improve body composition
- Enhance insulin sensitivity
- Reduce visceral fat
- Improve endothelial function
But it may also:
- Increase hematocrit
- Promote platelet aggregation in certain contexts
- Alter lipid fractions
The net effect likely depends on:
- Baseline cardiovascular health
- Dose
- Hematologic response
- Duration of therapy
Clinical evidence landscape
Randomized trials in properly selected hypogonadal men have generally not shown a dramatic increase in major adverse cardiac events.
However:
- Some observational data suggest increased thrombotic risk in certain populations.
- Risk may be higher during the first 3–6 months in susceptible individuals.
Practical implication: avoid initiating TRT immediately after recent myocardial infarction or stroke, and stabilize cardiovascular risk factors first.
Prostate considerations: growth versus cancer risk
Testosterone does not appear to initiate prostate cancer in eugonadal men. However, it can stimulate growth in androgen-sensitive tissue.
Key points:
- PSA typically rises modestly (e.g., 0.3–0.5 ng/mL) after initiation.
- Significant or rapid PSA rise warrants evaluation.
- TRT is contraindicated in active prostate cancer.
Referral triggers include:
- PSA >4.0 ng/mL
- PSA increase >1.4 ng/mL in 12 months
- Abnormal digital rectal exam
The “saturation model” suggests that prostate androgen receptors become saturated at relatively low testosterone levels, meaning supraphysiologic increases may not proportionally increase cancer risk—but monitoring remains mandatory.
Estradiol-related side effects
Because testosterone aromatizes into estradiol, some men experience:
- Gynecomastia
- Breast tenderness
- Fluid retention
- Emotional lability
Excessively low estradiol (often due to overtreatment with aromatase inhibitors) may cause:
- Joint pain
- Low libido
- Reduced bone density
Management should be symptom-guided rather than reflexively suppressing estradiol.
Dermatologic and cosmetic effects
Common mild side effects include:
- Acne
- Oily skin
- Increased body hair
- Scalp hair thinning in genetically predisposed men
These are dose-dependent and more common with higher serum peaks.
Fertility suppression and testicular atrophy
Exogenous testosterone suppresses LH and FSH, reducing:
- Intratesticular testosterone
- Sperm production
Prolonged suppression may cause:
- Oligospermia
- Azoospermia
- Reduced testicular volume
Recovery after discontinuation is possible but may take months and is not guaranteed in all cases.
Men desiring fertility should:
- Avoid TRT monotherapy
- Consider hCG-based stimulation
- Consult reproductive specialists before starting
Sleep apnea and fluid dynamics
TRT may worsen untreated obstructive sleep apnea by:
- Increasing upper airway edema
- Increasing erythrocytosis-related viscosity
Screen high-risk patients before initiation.
Psychological and behavioral changes
Most men experience improved well-being when properly dosed. However, supraphysiologic dosing may cause:
- Irritability
- Mood instability
- Impulsivity
These effects are uncommon at physiologic replacement doses.
Monitoring framework: practical structure
A structured monitoring plan typically includes:
Baseline
- Total testosterone
- LH/FSH
- CBC
- PSA
- Lipid panel
- Liver enzymes
3–6 months
- Testosterone level (timed appropriately for formulation)
- CBC
- PSA
- Symptom review
Annually
- CBC
- PSA
- Testosterone
- Cardiometabolic risk assessment
Dose adjustments should be driven by:
- Symptoms
- Hematocrit trends
- PSA behavior
- Estradiol-related symptoms
Risk–benefit equilibrium
The key principle is not whether TRT has risks—it does—but whether:
- The patient has confirmed deficiency
- Symptoms meaningfully impair quality of life
- Monitoring is structured and consistent
- Dosing remains physiologic
When these conditions are met, risk is generally manageable in appropriately selected patients.
Delivery methods compared: injections, gels, patches and pellets(1)(5)
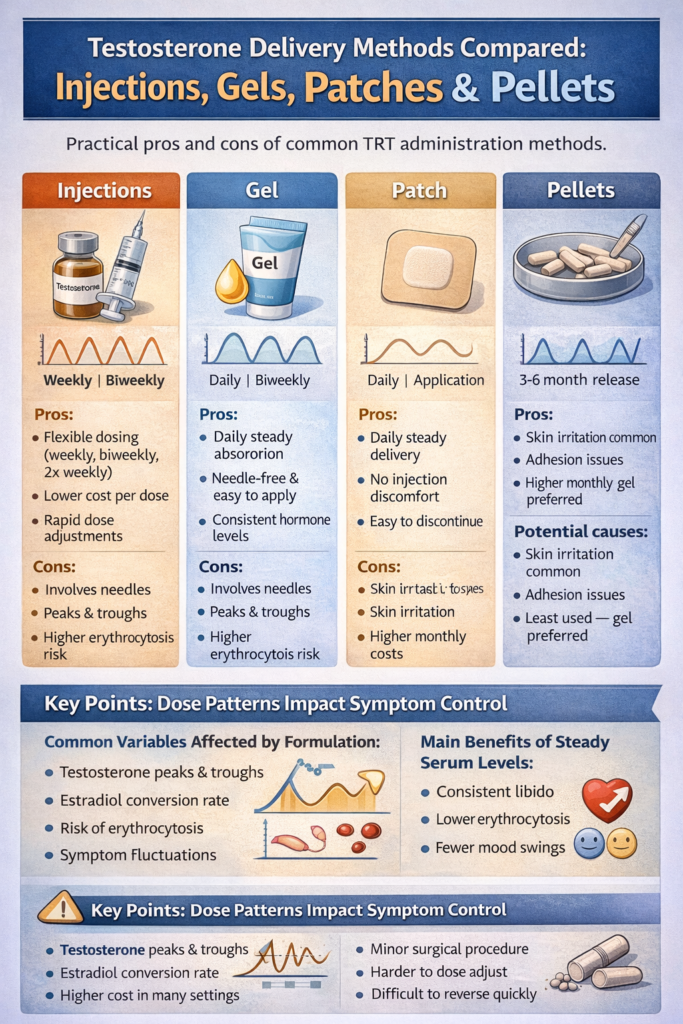
Delivery method affects convenience, cost, reversibility and blood-level stability, so choose a method that fits clinical goals and lifestyle. Practical differences between options can influence symptom control, monitoring frequency and out-of-pocket cost.
Intramuscular and subcutaneous injections offer flexibility and generally lower per-dose cost. Cypionate or enanthate injections are often given weekly to every two weeks and can produce higher peaks and lower troughs, while more frequent subcutaneous dosing, one to two times per week, tends to smooth levels and is suited to self-administration. Injections allow rapid dose adjustment, which helps when close monitoring is needed or when timing around fertility or competition is a consideration.
Transdermal gels and patches provide daily, steadier absorption and avoid needles, which many men prefer. Downsides include potential transfer to partners or children, skin irritation and often higher monthly cost for branded products.
Subdermal pellet implants release hormone over about three to six months after a minor office insertion and are low maintenance. They require a small procedure and are less easily reversed if side effects or fertility concerns arise.
Pharmacokinetics: why delivery method matters biologically
The primary difference between delivery systems is not just convenience—it is serum concentration dynamics.
Key variables influenced by formulation:
- Peak serum testosterone level
- Trough level before next dose
- Estradiol conversion rate
- Hematocrit stimulation intensity
- Symptom fluctuation
Stable physiologic exposure tends to produce:
- Fewer mood swings
- More consistent libido
- Lower erythrocytosis risk
- More predictable estradiol levels
Sharp peaks and troughs can amplify side effects in susceptible individuals.
Injectable testosterone: flexibility and potency
Intramuscular (IM) injections
Common esters:
- Testosterone cypionate
- Testosterone enanthate
These are oil-based depot preparations. After injection:
- Ester is slowly cleaved.
- Testosterone enters systemic circulation.
- Serum levels peak within 24–72 hours.
- Levels gradually decline over 7–14 days.
Weekly vs biweekly dosing
- Every 2 weeks: larger peaks, deeper troughs.
- Weekly dosing: smoother curve.
- Dividing into twice-weekly subcutaneous doses: even greater stability.
More frequent dosing often reduces:
- Mood variability
- Estradiol spikes
- Hematocrit acceleration
Subcutaneous injections
Lower-volume subcutaneous injections:
- Are well tolerated
- Produce stable pharmacokinetics
- Reduce injection-site discomfort for some men
Evidence suggests comparable serum levels to intramuscular dosing when total weekly dose is equivalent.
Advantages of injectables
- Lower cost
- Rapid dose titration
- Precise control of weekly exposure
- Easy to discontinue if needed
Disadvantages
- Needle-based
- Peak-trough variability if dosed infrequently
- Higher erythrocytosis risk at higher peaks
Injectables are often preferred when:
- Close laboratory titration is required
- Budget is a concern
- Patient is comfortable with self-administration
Transdermal gels and patches: steady-state physiology
Transdermal systems mimic more natural daily exposure patterns.
Mechanism
- Testosterone diffuses through the skin.
- Daily application maintains relatively stable serum levels.
- No large supraphysiologic peaks.
This often results in:
- Reduced hematocrit spikes
- More consistent estradiol levels
- Smoother mood profile
Advantages of gels
- Needle-free
- Stable serum levels
- Easy daily routine
- Lower risk of extreme peaks
Disadvantages
- Risk of transference to partners or children
- Skin irritation
- Variable absorption depending on skin characteristics
- Higher cost in many settings
Absorption can vary based on:
- Body fat distribution
- Skin thickness
- Application technique
Missed doses can cause more rapid level decline compared to long-acting injections.
Patches: less commonly used but stable
Transdermal patches provide:
- Controlled release over 24 hours
- Predictable pharmacokinetics
However, skin irritation rates are higher compared to gels, limiting long-term adherence.
Subdermal pellets: long-acting depot strategy
Pellets are implanted subcutaneously in a minor procedure.
Pharmacologic behavior
- Gradual release over 3–6 months
- Slow peak formation
- Long plateau phase
Advantages:
- Low maintenance
- No weekly dosing decisions
- High adherence
Limitations:
- Difficult to rapidly adjust dose
- Requires minor surgical procedure
- Harder to reverse quickly in case of side effects
- Potential local infection or extrusion
Pellets are best suited for:
- Stable, well-monitored patients
- Those prioritizing convenience
- Those with demonstrated stable dose requirements
Blood-level stability comparison (conceptual overview)
| Method | Peak Height | Stability | Dose Flexibility | Reversibility |
|---|---|---|---|---|
| Biweekly IM | High | Low | Moderate | High |
| Weekly IM | Moderate | Moderate | High | High |
| Split-dose SQ | Lower | High | Very high | High |
| Gel | Low | High | Moderate | High |
| Patch | Low | High | Moderate | High |
| Pellets | Moderate | High plateau | Low | Low |
The more flexible the system, the easier it is to adjust therapy based on laboratory trends and symptom feedback.
Choosing based on clinical scenario
Clinical situations favoring injections:
- Younger men
- Cost-sensitive patients
- Need for tight titration
- Hematocrit trending upward (allowing rapid adjustments)
Cases where gels may be preferred:
- Needle-averse patients
- Those sensitive to mood fluctuations
- Patients with prior erythrocytosis on injectables
When pellets may be preferred:
- Stable long-term therapy
- High adherence concerns
- Minimal desire for frequent medical contact
Estradiol and hematocrit behavior by formulation
Higher serum peaks (especially with large IM doses) may:
- Increase aromatization to estradiol
- Increase erythropoietin stimulation
- Elevate hematocrit more rapidly
Steady daily exposure (gels, divided injections) may:
- Produce more stable estradiol levels
- Reduce abrupt hematologic shifts
Individual enzymatic variability significantly influences these responses.
Reversibility and fertility implications
If fertility becomes urgent:
- Injectable and gel forms can be discontinued quickly.
- Pellets cannot be removed easily once implanted.
- Long-acting undecanoate injections (not discussed above but relevant) may persist longer.
Men concerned about fertility flexibility should consider shorter-acting modalities.
Practical decision framework
Choosing a delivery method should consider:
- Clinical stability
- Fertility goals
- Hematologic response history
- Budget
- Lifestyle and adherence patterns
- Tolerance for injections
No single method is universally superior. The optimal choice is the one that achieves:
- Stable physiologic testosterone levels
- Minimal side effects
- Sustainable long-term adherence
How to start TRT: tests, questions and finding a provider
Begin with a targeted history, physical exam and baseline testing. Recommended initial labs include a morning total testosterone, repeat total or free testosterone if results are borderline, LH and FSH to classify primary versus secondary causes, CBC with hematocrit, PSA with digital rectal exam when indicated, fasting lipid panel and liver function tests. Comprehensive reviews summarize diagnostic approaches and monitoring recommendations that help clinicians implement safe initiation and follow-up (comprehensive review).
Follow-up timing depends on formulation: check levels about one month after starting injectables for dose tuning, then at three to six months and every six to twelve months thereafter with ongoing symptom review. Repeat CBC at three to six months and then periodically, and repeat PSA at three to six months and annually if stable.
Bring a concise symptom checklist and a list of questions to your clinician. Ask whether you meet diagnostic criteria based on symptoms and repeat morning tests, which formulation fits your lifestyle, how treatment will affect fertility and what options preserve it, what monitoring schedule the clinician will use, and which signs should prompt immediate contact. Choose a licensed provider, such as primary care, urology or endocrinology, or use a verified telemedicine clinic with board-certified clinicians, and verify credentials and prescription authenticity before purchasing medications.
Clear next steps for understanding and pursuing TRT(1)
Start by scheduling a properly timed morning blood draw for total testosterone, ideally between 7:00 and 10:00 AM, and include SHBG if available. Document symptoms carefully—particularly sexual changes, energy decline, body composition shifts and reproductive concerns—before discussing treatment. Testosterone replacement therapy should only be considered after consistent biochemical confirmation and a structured clinical evaluation.
Testosterone deficiency is not defined by a number alone. It represents impaired androgen signaling within the hypothalamic–pituitary–gonadal axis, often accompanied by meaningful symptoms that affect sexual function, body composition, bone integrity, erythropoiesis and psychological well-being. Effective treatment requires more than prescribing hormone—it requires understanding physiology, identifying etiology and applying individualized dosing within a physiologic range.
Evidence shows that properly selected men with confirmed hypogonadism can expect consistent improvements in libido, modest gains in erectile function, measurable increases in lean body mass, gradual reductions in fat mass and long-term benefits in bone density. These improvements develop along predictable timelines and are most pronounced in men with clearly low baseline testosterone. TRT restores normal biologic signaling; it does not create supraphysiologic enhancement.
At the same time, therapy carries predictable risks. Erythrocytosis, fertility suppression and PSA changes require structured monitoring. Cardiovascular safety remains an area of active investigation, reinforcing the importance of individualized risk assessment. Dose matters. Delivery method matters. Monitoring discipline matters.
Choosing between injections, transdermal systems or pellets should be based on:
- Desired serum stability
- Need for dose flexibility
- Fertility planning
- Cost considerations
- Tolerance for procedural intervention
There is no universally superior formulation—only the one best aligned with clinical goals and patient context.
If treatment is recommended, confirm that it is prescribed by a licensed clinician, establish a laboratory follow-up schedule at three to six months and annually thereafter, and reassess both symptoms and objective markers regularly. Adjustments should be guided by physiologic response, not arbitrary target numbers.
Ultimately, responsible TRT is a long-term therapeutic relationship—not a short-term intervention. When properly diagnosed, carefully dosed and consistently monitored, testosterone replacement therapy can meaningfully restore health domains affected by androgen deficiency while maintaining safety through structured oversight.
The next step is not simply starting therapy. The next step is ensuring that diagnosis, expectations, monitoring and formulation choice are aligned from the beginning.
FAQ: What Is Testosterone Replacement Therapy for Men?
What Is Testosterone Replacement Therapy for Men?
Testosterone replacement therapy (TRT) is a medical treatment designed to restore testosterone to a physiologic mid-normal range in men with confirmed hypogonadism. It is indicated when clinically meaningful symptoms—such as reduced libido, erectile dysfunction, loss of muscle mass, fatigue, or decreased bone density—occur alongside consistently low morning testosterone levels on at least two separate laboratory tests.
TRT does not “boost” testosterone beyond normal biological limits. Its purpose is to restore proper androgen signaling within the hypothalamic–pituitary–gonadal axis while maintaining safety through structured monitoring.
What Is Testosterone Replacement Therapy for Men and How Does It Work?
Testosterone replacement therapy works by supplying exogenous testosterone to compensate for inadequate endogenous production.
Under normal physiology:
- The hypothalamus releases GnRH.
- The pituitary releases luteinizing hormone (LH).
- LH stimulates the testes to produce testosterone.
When this system is impaired, testosterone levels fall and symptoms develop. TRT bypasses this dysfunction by directly introducing testosterone into circulation. The hormone then binds to androgen receptors in muscle, bone, brain, and other tissues, supporting:
- Sexual function
- Muscle protein synthesis
- Bone mineral density
- Red blood cell production
- Metabolic regulation
However, exogenous testosterone suppresses LH and FSH through negative feedback, reducing natural testosterone production and sperm generation.
What Is the Best Testosterone Replacement Therapy for Men?
There is no single “best” testosterone replacement therapy for men. The optimal approach depends on:
- Clinical stability
- Fertility goals
- Hematocrit response
- Cardiovascular risk profile
- Lifestyle preferences
- Cost considerations
The most effective TRT regimen is one that restores physiologic levels, improves symptoms, minimizes side effects, and allows structured monitoring and dose adjustment.
What Is the Best Form of Testosterone Replacement Therapy for Men?
The best form of testosterone replacement therapy for men varies by individual. Available options include:
- Intramuscular injections (cypionate or enanthate)
- Subcutaneous injections
- Transdermal gels
- Transdermal patches
- Subdermal pellets
- Oral testosterone undecanoate (in select cases)
Injectables are flexible and cost-effective but may produce peak–trough fluctuations if dosed infrequently. Divided weekly or twice-weekly injections provide greater stability. Gels offer steady daily absorption but require careful application to prevent transfer. Pellets provide long-term release but are less easily adjustable.
The best form is the one aligned with physiologic stability, safety monitoring, and patient adherence.
What Are the Best FDA-Approved Testosterone Replacement Therapy Products for Men?
FDA-approved testosterone therapies include:
- Testosterone cypionate
- Testosterone enanthate
- Testosterone undecanoate
- Transdermal gels (various branded and generic options)
- Transdermal patches
- Subdermal pellets
All approved therapies aim to restore testosterone within a normal physiologic range. No product is universally superior; clinical suitability depends on individual response and risk profile.
What Are the Different Methods of Testosterone Delivery Available?
Testosterone can be delivered through:
- Intramuscular injections
- Subcutaneous injections
- Daily transdermal gels
- Transdermal patches
- Subdermal pellet implants
- Oral formulations (limited indications)
Each method differs in pharmacokinetics, peak concentration, serum stability, reversibility, and cost. Stable delivery methods may reduce estradiol fluctuations and hematocrit elevation in some men.
What Is the Process for Getting Prescribed Testosterone Replacement Therapy?
The process typically includes:
- Clinical evaluation of symptoms.
- Two separate morning total testosterone tests.
- Measurement of SHBG or free testosterone if levels are borderline.
- LH and FSH testing to determine primary vs secondary hypogonadism.
- Baseline CBC and PSA screening.
- Review of contraindications.
- Fertility discussion before therapy initiation.
TRT should not be prescribed based on a single lab result or symptoms alone.
Are There Clinics Near Me That Offer Testosterone Replacement Therapy for Men?
TRT is offered by:
- Primary care physicians
- Urologists
- Endocrinologists
- Men’s health specialty clinics
- Telemedicine hormone services
When searching locally, prioritize licensed clinicians who require laboratory confirmation and follow structured monitoring protocols.
How Do I Find a Reputable Clinic Offering Hormone Therapy for Men?
A reputable clinic should:
- Require repeat lab confirmation
- Conduct baseline PSA and hematocrit testing
- Discuss fertility implications
- Provide structured follow-up
- Avoid supraphysiologic dosing
Red flags include prescribing without labs, standardized high-dose protocols, and lack of physician supervision.
Are There Online Services for Testosterone Level Assessment and Treatment?
Yes, telemedicine platforms offer remote consultations, coordinated lab testing, and prescription fulfillment. However, responsible services should still:
- Require proper diagnostic confirmation
- Screen for contraindications
- Provide physician oversight
- Maintain structured follow-up monitoring
Convenience should not replace clinical rigor.
How Much Does Testosterone Replacement Therapy Cost on Average in the US?
Costs vary depending on formulation and provider model.
Approximate monthly ranges:
- Injectable testosterone (generic): $30–$150
- Transdermal gels: $200–$500+
- Pellets: $500–$1,500 per insertion cycle
- Telemedicine programs (including labs): $100–$300
Insurance coverage varies, and monitoring labs add to total cost.
Compare the Costs of Various TRT Treatment Options
Injectables:
Lowest medication cost, flexible dosing, additional supply costs.
Transdermal gels:
Higher monthly cost, no injection supplies, stable serum levels.
Pellets:
Higher upfront cost, low maintenance, limited reversibility.
Cost should be weighed against long-term monitoring quality and clinical oversight.
Which Companies Provide Testosterone Replacement Therapy Services for Men?
TRT services are provided by:
- Hospital-based practices
- Private urology and endocrinology clinics
- Men’s health centers
- Licensed telemedicine hormone providers
When evaluating providers, prioritize medical oversight, lab requirements, transparency, and adherence to physiologic dosing principles.
What Is the Best Testosterone Replacement Therapy for Men Over 40?
For men over 40, treatment should be based on confirmed hypogonadism—not age alone. Stable dosing strategies and structured cardiovascular risk assessment are particularly important in this population.
What Is the Best Testosterone Replacement Therapy for Men With Fertility Concerns?
Standard TRT suppresses spermatogenesis. Men who wish to preserve fertility should discuss alternatives such as:
- hCG-based stimulation
- Selective estrogen receptor modulators
- Combination regimens under specialist care
Fertility planning should occur before starting therapy.
What Is the Best Testosterone Replacement Therapy for Men Overall?
The best testosterone replacement therapy for men is:
- Medically indicated
- Confirmed by repeat laboratory testing
- Dosed within physiologic range
- Closely monitored
- Individualized to clinical goals
Successful TRT is defined by symptom improvement with stable laboratory markers—not by achieving supraphysiologic testosterone levels.
References What Is Testosterone Replacement Therapy for Men
- Bhasin, S., Brito, J. P., Cunningham, G. R., Hayes, F. J., Hodis, H. N., Matsumoto, A. M., Snyder, P. J., Swerdloff, R. S., Wu, F. C. W., & Yialamas, M. A. (2018).
Testosterone therapy in men with hypogonadism: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 103(5), 1715–1744.
https://academic.oup.com/jcem/article/103/5/1715/4939465 - Ponce, O. J., Spencer-Bonilla, G., Alvarez-Villalobos, N., Serrano, V., Singh-Ospina, N., Rodriguez-Gutierrez, R., Salcido-Montenegro, A., Benkhadra, R., Prokop, L. J., Bhasin, S., & Brito, J. P. (2018).
The efficacy and adverse events of testosterone replacement therapy in hypogonadal men: A systematic review and meta-analysis of randomized, placebo-controlled trials. Journal of Clinical Endocrinology & Metabolism, 103(5), 1745–1754.
https://doi.org/10.1210/jc.2018-00404 - American Academy of Family Physicians (2024).
Testosterone replacement therapy for male hypogonadism. American Family Physician, 109(6), 543–549.
https://www.aafp.org/pubs/afp/issues/2024/0600/testosterone-replacement-therapy-male-hypogonadism.html - Seal, L. J. (2025).
Male hypogonadism and testosterone replacement therapy. Medicine, 53(10), 638-643.
https://www.sciencedirect.com/science/article/pii/S1357303925001823 - Mulhall, J. P., Trost, L. W., Brannigan, R. E., Kurtz, E. G., Redmon, J. B., Chiles, K. A., Lightner, D. J., Miner, M. M., Murad, M. H., Nelson, C. J., & Parish, S. J. (2018).
Evaluation and management of testosterone deficiency: AUA guideline. The Journal of Urology, 200(2), 423–432.
https://www.auanet.org/guidelines/testosterone-deficiency-guideline - Braga, J., et al. (2025). (review)
Rhythm, risk, and responsibility: Assessing the safety of testosterone therapy. Journal of Clinical Outcomes in Men’s Health. Springer Nature.
https://link.springer.com/article/10.1007/s40256-025-00763-8 - The Lancet Healthy Longevity (2023).
Symptomatic benefits of testosterone treatment in patient subgroups: A systematic review and meta-analysis. The Lancet Healthy Longevity.
https://www.thelancet.com/journals/lanhl/article/PIIS2666-7568(23)00169-1/fulltext - National Institute for Health and Care Research. (2023).
Research provides reassurance about the safety of testosterone treatment. NIHR Evidence.
https://evidence.nihr.ac.uk/alert/research-provides-reassurance-about-the-safety-of-testosterone-treatment/ - U.S. Food and Drug Administration. (2015; updated 2025).
FDA drug safety communication: Testosterone products — labeling changes regarding cardiovascular risk. FDA.
https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-testosterone-products-drug-labeling-change-required - UpToDate (2026).
Testosterone treatment of male hypogonadism. UpToDate clinical topic review.
https://www.uptodate.com/contents/testosterone-treatment-of-male-hypogonadism
Leave a Reply