Most Popular steroids USA
-
 Trenbolone 200 20ml - Sydgroup
$53.00
Trenbolone 200 20ml - Sydgroup
$53.00 -
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
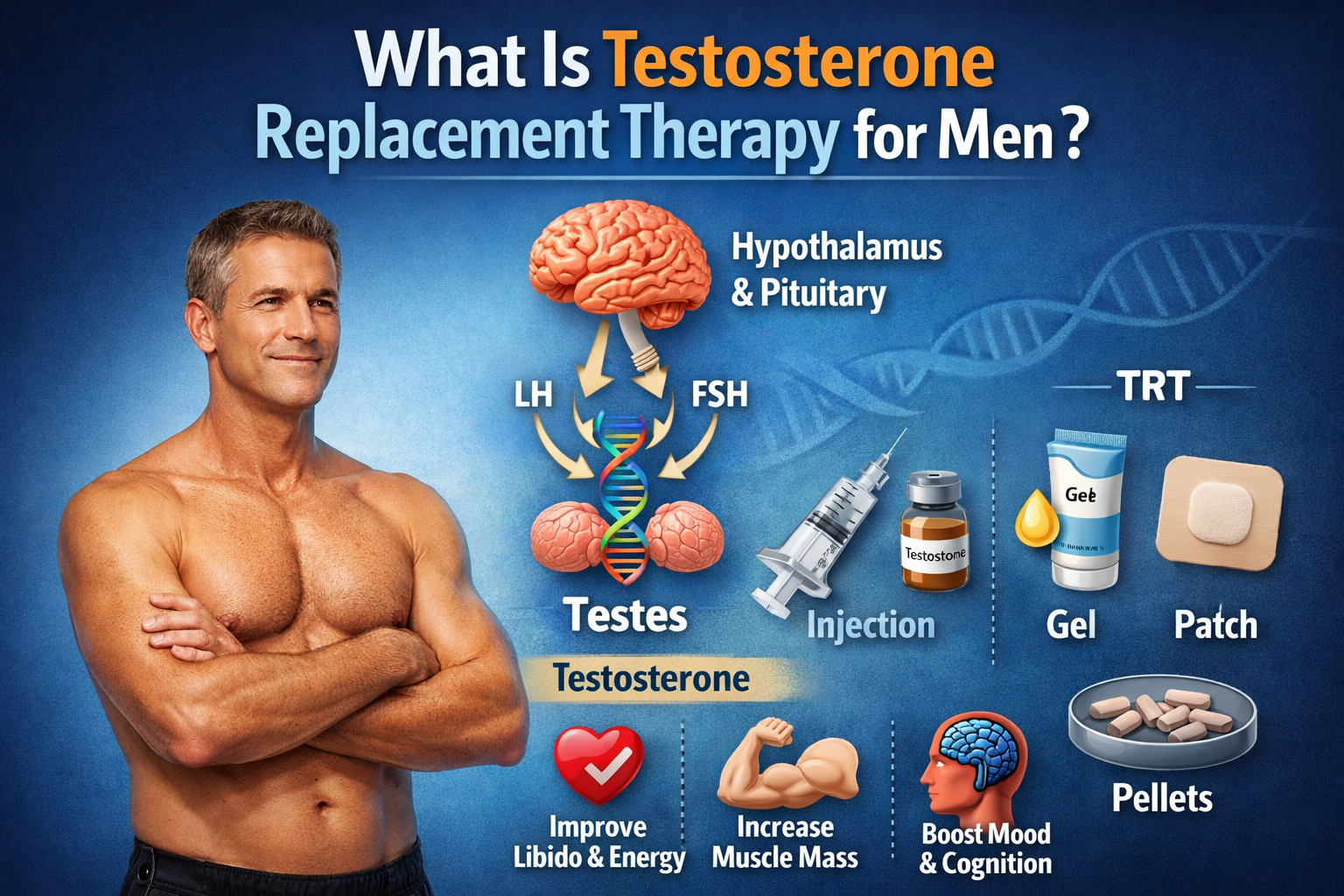
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
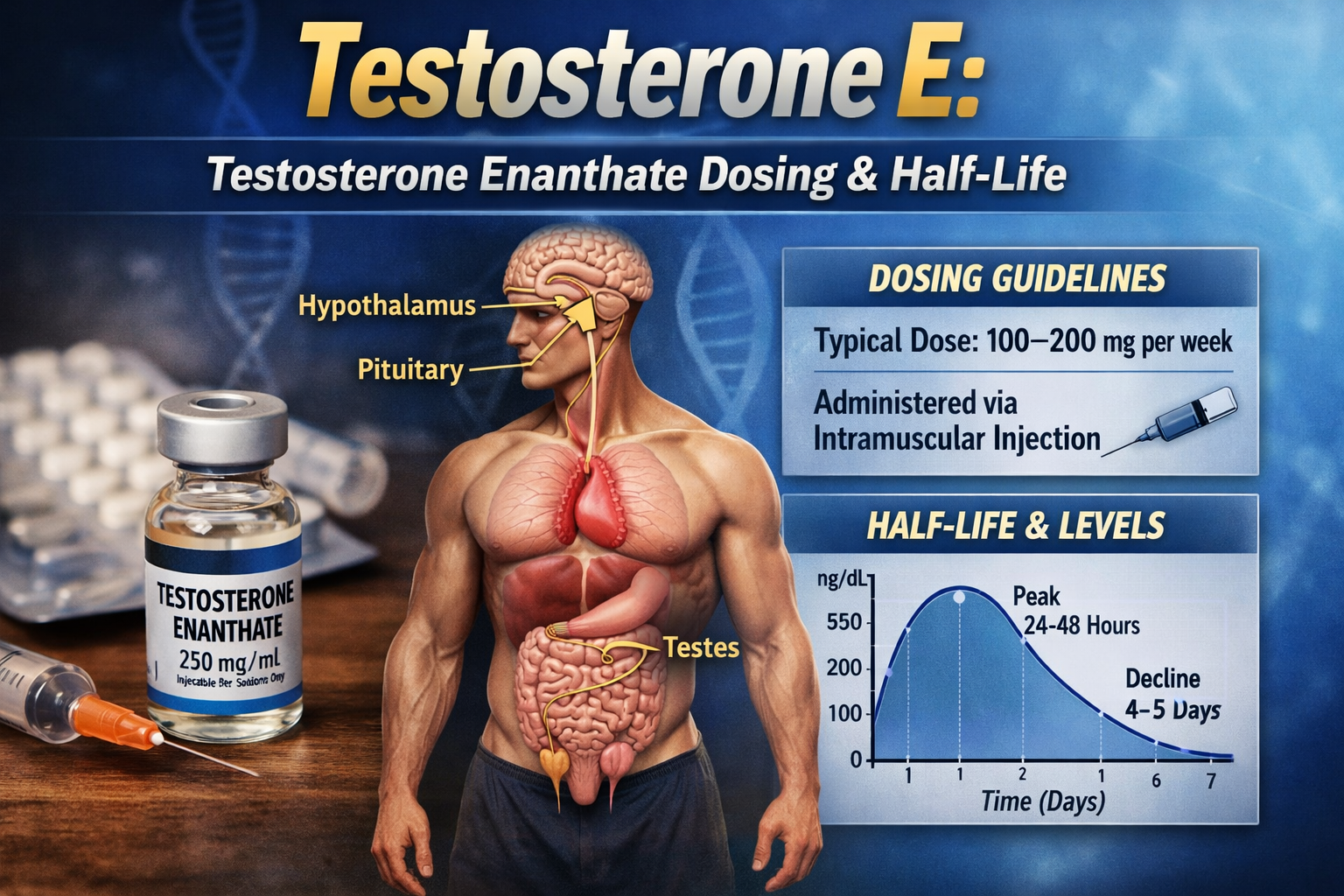
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.