Most Popular steroids USA
-
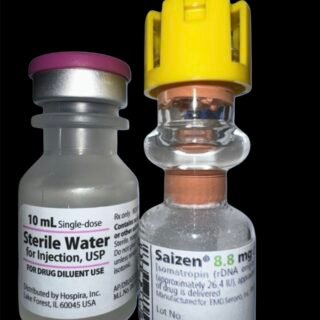
 Saizen 8.8 mg (Somatropin) 26.4 UI Domestic USA
Original price was: $115.00.$98.00Current price is: $98.00.
Saizen 8.8 mg (Somatropin) 26.4 UI Domestic USA
Original price was: $115.00.$98.00Current price is: $98.00. -
PARAMIX 300 Genli Pharma – Trenbolone A, E & Hexa Mix 10 ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Drostanolone Enanthate 200mg 10 ml - Masteron Enanthate
Original price was: $110.00.$90.00Current price is: $90.00.
-
Primobolan Pills 25mg 100 pills Domestic USA
Original price was: $99.00.$85.00Current price is: $85.00.
-
Clenbuterol for Sale 40mcg 100 Tabs - GP Premium Domestic USA
Original price was: $99.00.$65.00Current price is: $65.00.





Saizen 8.8 mg (Somatropin) 26.4 UI Domestic USA
Original price was: $115.00.$98.00Current price is: $98.00.
Saizen 8.8 mg (Somatropin) is a recombinant human growth hormone designed for the treatment of growth hormone deficiency (GHD) in both children and adults. Each vial contains 8.8 mg (approximately 26.4 IU) of somatropin, a bio-identical form of natural GH that supports tissue growth, metabolism, and recovery. The lyophilized powder must be reconstituted with bacteriostatic water and administered via subcutaneous injection. Clinically, Saizen helps stimulate linear growth in pediatric patients and improves body composition, muscle mass, and energy levels in adults with GHD. Manufactured by EMD Serono, it is recognized for its purity, safety, and reliable performance in hormone replacement therapy.
Saizen 8.8 mg (Somatropin): Clinical Uses, Dosing, and Off-Label Bodybuilding Use
Saizen 8.8 mg is a brand of recombinant human growth hormone (somatropin) used to treat growth hormone deficiency (GHD). The 8.8 mg presentation refers to a lyophilized powder vial containing 8.8 mg of somatropin (approximately 26.4 IU of GH) per vial (fda.gov). When reconstituted, Saizen is administered by injection to supplement or replace endogenous growth hormone. Below, we detail Saizen’s approved clinical uses in children and adults with GHD, dosing and administration protocols (including reconstitution and monitoring), and its off-label use in bodybuilding (with associated dosing practices, purported effects, and risks).
Clinical Uses in Growth Hormone Deficiency
Pediatric Patients (Children and Adolescents)
Saizen 8.8 mg is indicated for the long-term treatment of children with growth failure due to inadequate secretion of endogenous growth hormone (fda.gov). In clinical practice, this means pediatric patients diagnosed with GHD – whether due to congenital, genetic, idiopathic, or acquired causes – can be prescribed Saizen to promote linear growth. Treatment is typically initiated after confirmation of GH deficiency (often via stimulation testing) and is continued through childhood until the child’s epiphyseal growth plates fuse (i.e. when the child’s bones have finished growing) (fda.gov). The goal in pediatric use is to normalize height velocity and help the child achieve an adult height in the expected range for their family. It’s important to note that Saizen’s approved pediatric indication is specifically for growth failure from proven GH deficiency; it is not labeled (in the U.S.) for other causes of short stature such as Turner syndrome, idiopathic short stature, or small-for-gestational-age without catch-up growth – indications which some other somatropin products have, but Saizen does not (alaska.gov). (Clinicians may still use Saizen for such conditions off-label, but those are not FDA-approved indications.)
Therapy in children is monitored by periodic height measurements and IGF-1 levels to ensure an adequate response. If a child shows lack of response (poor growth velocity), adherence and other causes (like hypothyroidism or neutralizing GH antibodies) should be evaluated (fda.gov). Once the child’s epiphyses have fused (or if treatment fails to be effective), therapy is discontinued (fda.gov).
Adult Patients (Growth Hormone Deficient Adults)
In adults, Saizen is indicated as replacement therapy for adults with confirmed growth hormone deficiency. This includes two groups: adult-onset GHD, often due to pituitary or hypothalamic disease or injury (e.g. pituitary tumors, surgery, radiation, or trauma), and childhood-onset GHD where an individual treated for GHD in childhood is retested in adulthood and still found to be deficient (fda.gov). Generally, an adult patient must meet clinical criteria for GHD and have failed a GH stimulation test to be eligible for treatment (fda.gov). The purpose of GH replacement in adults is to improve body composition, physical capacity, and quality of life in those with true hormone deficiency. Studies in GH-deficient adults have shown that restoring GH to physiologic levels can increase lean body mass and bone density, reduce fat mass, and improve exercise tolerance and some aspects of cardiovascular health (pmc.ncbi.nlm.nih.gov). Patients often report improved energy and wellbeing once an appropriate dose is established.
Adult GHD treatment is not intended for healthy elderly or “anti-aging” purposes and is only indicated for diagnosed hormone deficiency. Prior to starting therapy, any active malignancy must be ruled out, and if the adult GHD is due to a pituitary tumor, that disease should be stable (e.g. adequately treated) before initiating GH. Like in pediatric use, adult patients on GH are monitored (clinical symptoms and IGF-1 levels) and dosing is adjusted to avoid excess levels. Adult GH therapy is typically lifelong, unless the deficiency is transient or another cause intervenes.
Saizen 8.8 mg (Somatropin) Dosing and Administration Protocols
Dosing of Saizen must be individualized for each patient, with pediatric dosing based primarily on weight and adult dosing starting low and titrating to effect. The following table summarizes typical dosing recommendations for children and adults with GHD:
💉 Saizen 8.8 mg (≈ 26.4 IU) — Dosing Guidelines
| Patient Population | Recommended Dose & Regimen | Approximate IU Equivalent | Administration Route / Frequency | Treatment Duration & Monitoring |
|---|---|---|---|---|
| Children with GHD | 0.18 mg/kg per week of somatropin, divided into 6–7 doses (≈ 0.03 mg/kg daily). Example: 20 kg child ≈ 3.6 mg/week → ≈ 10.8 IU/week → ~1.8 IU/day. | ~3 IU per mg → Each mg = 3 IU. Typical child (20 kg): ≈ 10–12 IU/week total. | Subcutaneous (SC) injection, preferably daily (6 days per week or daily). SC is preferred; IM acceptable if needed. | Treat until linear growth is complete (epiphyses fused). Monitor height velocity, IGF-1 levels, and clinical response. Adjust dose as needed; discontinue when growth stops or goals are achieved. |
| Adults with GHD | Start ~ 0.2 mg/day (≈ 0.6 IU/day); after ≈ 4 weeks, increase toward ≤ 0.01 mg/kg/day (≈ 3 IU/day) if tolerated. Alternatively, start 0.15–0.3 mg/day (≈ 0.45–0.9 IU/day) and titrate up by 0.1–0.2 mg (≈ 0.3–0.6 IU) every 1–2 months. | Typical maintenance range ≈ 0.6–3 IU/day. Younger or female patients (often on estrogen) may require higher IU within this range. | Subcutaneous injection once daily — often in the evening or at bedtime to mimic the natural GH nocturnal surge. | Long-term therapy (years or lifelong). Monitor IGF-1 (keep within age-adjusted normal range), clinical symptoms, and side effects. Adjust dose downward if intolerance or IGF-1 above normal. Evaluate periodically for efficacy in body composition and well-being. |
Pediatric dosing: As shown above, children receive weight-based dosing of roughly 0.18 mg per kg body weight per week (fda.gov). This weekly total is typically divided into daily injections for convenience and better efficacy. A common schedule is daily SC injections 6 days per week (with one rest day) or every day; older regimens sometimes used 3 injections per week, but daily administration yields more consistent growth stimulation (fda.gov). For example, a 30 kg child would receive about 5.4 mg of GH per week, given as ~0.9 mg per day. The dose may be adjusted based on the child’s response and IGF-1 levels. During periods of rapid growth or puberty, higher doses (within safe limits) may be considered to maximize height outcomes, whereas if IGF-1 levels rise above the normal range for age, the dose should be reduced. Dosing in certain special pediatric populations (e.g. those with concomitant diabetes or Turner syndrome) might be conservative to start, due to higher risk of side effects (see Monitoring and Safety below). Importantly, once the child’s growth plates have closed, further GH therapy will not increase height and should be stopped (fda.gov).
Adult dosing: Adults with GHD are started at a low dose and titrated carefully. A typical starting dose is 0.1–0.2 mg per day (which in many cases is ≤0.005 mg/kg/day). After about 4 weeks, the dose can be gradually increased – for example to 0.3 mg/day, then 0.4 mg/day, and so on – up to around 0.01 mg/kg/day (depending on tolerability). Another recommended approach is to start at ~0.2 mg/day and uptitrate by ~0.1–0.2 mg every 1–2 months. The rationale is to “start low and go slow” – mitigating side effects in adults, who are more sensitive to GH’s fluid-retaining and metabolic effects. Maintenance doses vary widely from person to person; younger adults and women on oral estrogen tend to need higher doses, whereas older or overweight patients may require lower doses for safety. During dose titration, serum insulin-like growth factor 1 (IGF-1) is measured and the dose adjusted to achieve an IGF-1 level in the normal range for the patient’s age and sex. Clinical symptoms and side effects are also monitored closely. Many adult patients end up on maintenance doses in the range of ~0.2 mg to 1 mg daily, depending on their individual sensitivity and needs. If excessive side effects occur (see Monitoring and Safety), the dose is reduced. Adult GH therapy is a long-term treatment; there is no predefined “course length” – rather, the hormone deficiency is chronic, so therapy continues indefinitely as long as benefits continue and no contraindications emerge.
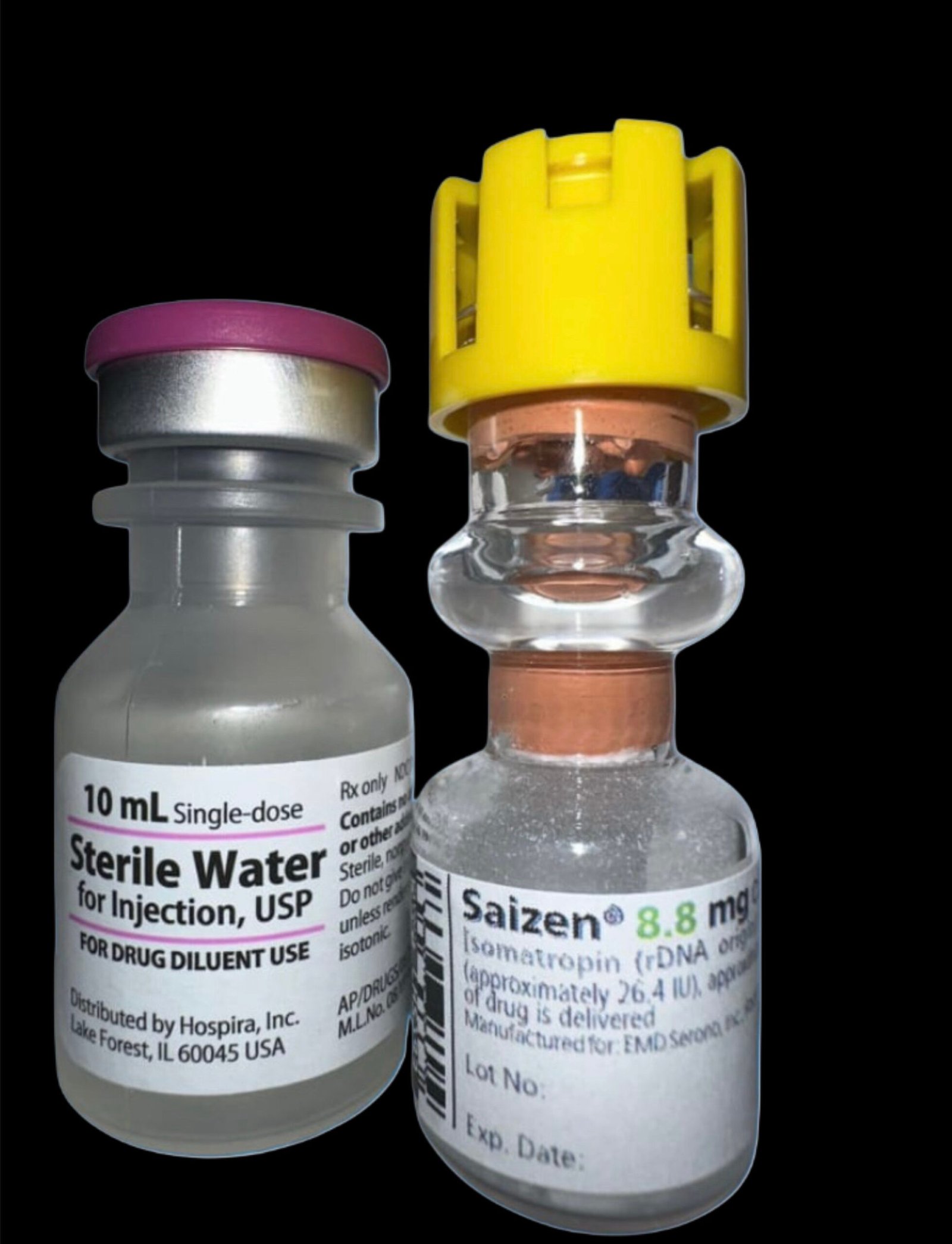
Saizen 8.8 mg Preparation and Reconstitution
Saizen comes as a sterile lyophilized powder. Before injection, the user must mix it with the supplied diluent. To prepare an 8.8 mg vial of Saizen, dissolve the powder in 2–3 mL of Bacteriostatic Water for Injection (0.9% benzyl alcohol). Using 2 mL produces a higher concentration, while 3 mL makes it easier to draw doses; the prescribing information permits either volume. When adding the diluent, direct the liquid stream against the glass wall of the vial rather than onto the powder. Swirl the vial gently in a rotary motion until the powder fully dissolves. Avoid shaking it, as vigorous agitation can denature the protein and make the solution cloudy. You should obtain a clear solution. Check for any particles or cloudiness. If the solution looks cloudy or contains undissolved flakes, discard it. (A few small, colorless particles may appear after refrigeration; they usually dissolve once the solution warms to room temperature.)
Patients who cannot tolerate benzyl alcohol (such as neonates or those with a benzyl alcohol allergy) should mix Saizen with sterile water instead. However, they must use the solution immediately and avoid storing it, since it contains no preservative.
After mixing, handle storage and stability carefully. When you reconstitute a multi-dose vial with bacteriostatic water, store it in the refrigerator at 2–8 °C. Saizen 5 mg and 8.8 mg vials mixed with benzyl-alcohol diluent remain stable for up to 14 days under refrigeration.
Injection Administration in Saizen 8.8 mg
Saizen is administered by subcutaneous injection, and this route is preferred for consistency and tolerability. Patients (or caregivers) typically inject the hormone into a fatty subcutaneous area, such as the thigh, buttocks, upper arm, or abdomen (avoiding the navel area). Injection sites should be rotated to prevent lipoatrophy or irritation at any one location. While SC injections are most common, Saizen can also be given by intramuscular (IM) injection if needed. (IM administration may be used in cases where SC is not feasible; however, SC provides more gradual absorption and is generally recommended.) The injections are usually given in the evening or at bedtime for adults (to coincide with the body’s natural GH secretion cycle), whereas in children the timing can be less critical but is often done in the evenings as well.
Administration requires using insulin syringes or pen needles (for the Saizen pen device) to measure the small doses accurately. Patients should be thoroughly instructed on injection technique. Example: For a child needing a 0.5 mg dose from a reconstituted vial at 8.8 mg/2 mL concentration (i.e. 4.4 mg/mL), the volume to inject would be ~0.11 mL. The small volumes underscore the importance of proper syringe usage to measure doses. As Saizen therapy is often long-term, many patients use injection devices (pen injectors) that can simplify dosing – the Saizen easypod® is an electronic auto-injector designed for Saizen cartridges, which can automate dose measurement and track injection history (though detailed discussion of devices is beyond our scope).
Monitoring and Safety Considerations
Patients on Saizen require regular monitoring to ensure efficacy and detect adverse effects early.
Growth and IGF-1:
The primary efficacy markers are linear growth (height gain) in children and IGF-1 levels (in both children and adults). Pediatric patients should have height and weight tracked at least every 3–6 months, with dose adjustments if growth velocity is inadequate. Serum IGF-1 can be measured to confirm that the dose is achieving physiological levels; an IGF-1 level kept within the age-appropriate normal range is a target to avoid under or over-dosage. In adults, IGF-1 is checked 4–8 weeks after dose changes and periodically thereafter. The clinical response is also important – improvements in symptoms (energy, stamina) and body composition support continuing therapy.
Metabolic monitoring:
Growth hormone can affect glucose metabolism. It tends to cause insulin resistance with chronic use, which in some patients can lead to impaired glucose tolerance or even new-onset type 2 diabetes. Patients with risk factors for diabetes (e.g. obesity, family history, or concomitant steroids) should have blood glucose monitored more frequently. Fasting blood sugar or HbA1c may be assessed periodically. In fact, GH should be used cautiously or at lower doses in patients with diabetes, and their anti-diabetic medications might require adjustment when GH therapy is initiated. (During GH therapy, one might see initial hypoglycemia followed by hyperglycemia as a rebound effect, and long-term high doses clearly increase diabetes risk.) For example, clinical guidelines note that children with certain syndromes (like Turner or Prader-Willi) or a family history of diabetes should be watched closely for glucose changes. Overall, while standard pediatric doses rarely cause diabetes, the risk becomes more pertinent at the higher doses sometimes misused in bodybuilding (discussed later).
Thyroid function:
GH and thyroid hormones are interrelated, and GH therapy can unmask or worsen hypothyroidism in individuals with underlying thyroid issues. In GHD patients (especially those with panhypopituitarism), starting GH may increase peripheral conversion of T4 to T3, reducing T4 levels and revealing a central hypothyroidism that was previously subclinical. Undiagnosed hypothyroidism can blunt the growth response to GH. Thus, periodic thyroid function tests (TSH, free T4) are recommended for both children and adults on long-term GH therapy. If the patient has primary or secondary hypothyroidism, it should be adequately treated with thyroid hormone for optimal results.
IGF-1 and other labs:
Besides IGF-1, GH can raise levels of markers like alkaline phosphatase and inorganic phosphorus due to its effects on bone turnover. These are generally not harmful and reflect the anabolic action on bone. Pediatric patients who are growing rapidly on GH should have scoliosis checks, as GH can accelerate growth and occasionally worsen pre-existing spinal curvature. Another rare but serious side effect in children is intracranial hypertension (pseudotumor cerebri) – typically presenting with headache, visual changes, or papilledema. This usually occurs within the first 8 weeks of therapy if it’s going to happen. If a patient complains of severe headaches or vision problems, an eye exam for papilledema should be done. GH should be stopped if intracranial hypertension is confirmed, and can be resumed at a lower dose after it resolves (data.fda.gov.) Fortunately, this side effect is uncommon.
General safety:
Growth hormone acts as a powerful growth-promoting agent, so clinicians must avoid prescribing it to patients with active malignancies. Doctors should confirm that any pre-existing tumor, especially a pituitary tumor, remains stable or in remission before treatment. Childhood cancer survivors who receive GH require ongoing monitoring for possible recurrence. The Saizen label reports some cases of secondary neoplasms—such as secondary brain tumors—among childhood cancer survivors treated with GH, although studies have not established a direct causal link. Physicians should schedule regular follow-ups for all patients, particularly those with a cancer history, to detect early signs of tumor return. Clinicians must also avoid starting GH therapy during any critical illness, such as an ICU stay after major surgery or trauma, because high-dose GH in these situations has been shown to raise mortality. In addition, doctors should not prescribe GH to patients with Prader-Willi syndrome who are severely obese or experience breathing problems, since reports have linked such cases to sudden death, especially when eligibility criteria were not properly followed.
Adverse effects:
Common side effects of GH therapy include edema (fluid retention), joint pain or muscle aches, carpal tunnel syndrome (nerve compression in the wrist causing tingling in the hands), and headaches. These tend to be dose-related and more frequent in adults than children. If dosing is appropriately titrated, children usually tolerate GH very well with few side effects, whereas adults – especially older adults – might develop edema, arthralgias, or paresthesias that require dose reduction. In the long term, excessive GH dosing can produce symptoms resembling acromegaly (the condition of GH excess), such as enlargement of the extremities, coarse facial features, excessive sweating, and insulin resistance. However, at the proper replacement doses used for GHD, these effects are unlikely – they are mainly a concern in abuse situations or accidentally prolonged overdosing.
Patients should be educated about signs of serious adverse events: severe headaches (possible intracranial hypertension), hip or knee pain in children (possible slipped capital femoral epiphysis during rapid growth), or abdominal pain (pancreatitis has been reported rarely). Overall, when used at prescribed doses for indicated conditions, somatropin has a favorable safety profile and significantly benefits patients with growth hormone deficiency. The following section will contrast this with unapproved uses where doses often far exceed therapeutic levels, leading to greater risks.
Saizen 8.8 mg Off-Label and Non-Medical Uses: Bodybuilding and Athletic Performance
Outside of its medical indications, human growth hormone (HGH) like Saizen has been used (illicitly) by some bodybuilders, athletes, and individuals seeking anti-aging or physique enhancement. These off-label uses are not sanctioned by medical guidelines due to uncertain efficacy and significant risks. Nonetheless, in the bodybuilding community, GH is often regarded as a powerful anabolic and fat-burning agent. This section examines typical dosing practices in that context, the purported effects, and the health risks associated with GH abuse.
Saizen 8.8 mg Dosage and Regimens in Bodybuilding
Typical doses:
Bodybuilders generally administer somatropin in doses much higher than those used in GH-deficient patients. Whereas a GH-deficient adult might use around 0.2–0.5 mg per day (equivalent to ~0.6–1.5 IU), a healthy bodybuilder might use several IU per day. Common regimens reported in forums and doping surveys are on the order of 2–4 IU daily for novices or for fat loss, up to about 6–8 IU daily for more advanced muscle-building purposes insidebodybuilding.com. Some elite or professional bodybuilders have reportedly pushed doses even higher (10+ IU per day), but high doses greatly increase side effects. To put this in perspective, 1 IU of GH is approximately 0.33 mg of somatropin. Thus, a 6 IU/day dose corresponds to ~2 mg of GH daily – which is 4–5 times the full replacement dose for a large adult male with GH deficiency.
A survey of doping practices in athletes found that regimens can involve 10–25 IU per day, administered 3–4 times per week in cycles. Often, users combine GH with anabolic steroids or other performance-enhancing drugs – the idea is that GH will increase lean mass and fat loss synergistically. One analysis noted the “underground” practice where the average GH dose (when spread over time) was about 4 IU per day, typically stacked with steroids in strength sports. Because GH is expensive and in limited supply, athletes sometimes do not take it daily year-round, but rather use it in cycles. A common cycle length might be 8–12 weeks of daily (or near-daily) use, often aligned with a training or competition cycle, followed by some weeks off. Some protocols involve injecting GH daily but with weekly “off-days” (e.g. the “5 days on, 2 days off” pattern) to potentially reduce tolerance and save cost – though the medical rationale for this is anecdotal. Others may inject GH only on training days (e.g. 3–4 days a week) at higher doses each time. In all cases, these dosing patterns are empirical and not scientifically validated; they evolved in the bodybuilding subculture and vary widely among individuals.
Saizen 8.8 mg Administration:
Off-label users administer GH subcutaneously, just as medical patients do. Injections are often timed either first thing in the morning or post-workout and/or before bed. Some split the total daily dose into two injections (morning and evening) to try to mimic natural pulsatile secretion and improve absorption. Others prefer a single larger dose once a day. There is debate in bodybuilding circles about optimal timing (e.g. pre-workout to aid training vs. before sleep to augment the nighttime GH peak, or morning to avoid interference with natural night peak). No consensus exists, and any approach is based on theory and personal experience rather than controlled studies.
Users also frequently combine GH with insulin and IGF-1 analogues in high-level bodybuilding, attempting to maximize anabolism. For example, a bodybuilder might use GH daily along with insulin injections post-workout and anabolic steroids; this dangerous polypharmacy is intended to mimic the hormonal milieu of extreme muscle growth. Again, these practices carry significant risks (insulin shock, organ stress) and have not been rigorously studied.
Saizen 8.8 mg Reported Effects and Perceived Benefits
Bodybuilders and athletes who use GH off-label do so for two main goals: increasing muscle mass/strength and reducing body fat. Growth hormone has well-known lipolytic (fat-burning) effects – it mobilizes fat from adipose tissue – and users indeed often observe body fat reduction and a leaner appearance on GH. It also causes an increase in lean body mass, which includes not just muscle but also water (GH causes fluid retention) and connective tissue. Many users report that GH “fills out” their muscles, increases vascularity, and improves recovery from workouts. Some anecdotal claims include: improved workout recovery and injury healing, slight increases in muscle size and strength, and a “tighter” look due to fat loss around the abdomen. GH is also thought to have an anti-catabolic effect, protecting muscle during calorie deficits (dieting/cutting phases).
However, the actual muscle-building (anabolic) effect of GH in an otherwise healthy athlete is less dramatic than anabolic steroids. Scientific studies on healthy weight-training adults have generally found that GH increases fat-free mass but much of that is water or connective tissue, with no significant gain in muscle strength (clinician) . One review noted that while high-dose GH can increase muscle size (volume), it may not improve actual muscle strength or exercise capacity, and in some cases can worsen endurance capacity (tga.gov.au). The strength gains reported anecdotally by bodybuilders likely come primarily from concurrent steroid use; it’s difficult to isolate GH’s contribution. Some controlled trials in athletes showed increases in lean mass but no greater improvements in muscle force compared to placebo. Nonetheless, bodybuilders often subjectively feel that GH “rounds out” their muscles and helps burn stubborn fat, especially when preparing for competitions. GH can also cause a mild diuretic effect (via sodium and water handling changes), which can make the user appear more defined. There are also off-label users in the anti-aging sphere who claim improved skin tone, fewer wrinkles, and increased vitality on low-dose GH – but these claims are largely anecdotal and controversial.
In summary, many bodybuilders believe GH increases muscle size (through cell volume expansion and possibly fiber hyperplasia), reduces fat mass, and enhances recovery. Users often claim that GH helps heal cartilage or connective tissue injuries because GH and IGF can stimulate collagen synthesis. For this reason, some older athletes use it to “lubricate joints” or speed up recovery, although research has not quantified these effects well. A psychological factor also plays a role: since GH is a banned and expensive drug, users often expect dramatic results, which can shape their perception of its benefits. Studies have not clearly proven that GH directly improves strength or power, and any gains likely occur indirectly through fat loss, placebo effects, or concurrent training improvements.
Saizen 8.8 mg Risks and Side Effects of GH Abuse
Using growth hormone without medical necessity and at supraphysiologic doses comes with significant risks. Many side effects are essentially symptoms of acromegaly (the condition of chronic GH excess). Notably, these risks increase with higher doses and longer duration of abuse:
Edema and joint disorders:
High-dose GH causes pronounced fluid retention, leading to edema (swelling in ankles, fingers, face). This can in turn cause joint stiffness and pain. Carpal tunnel syndrome is very commonly reported by bodybuilders on GH – numbness/tingling in the hands due to swollen tissue compressing the median nerve. In studies, up to CTS and arthralgias are dose-limiting side effects, even causing participants to withdraw. Swollen joints and muscle compartments can actually reduce mobility or strength, counteracting some training efforts.
Metabolic disturbances:
Chronic GH elevates blood sugar by inducing insulin resistance. Hyperglycemia and eventually diabetes mellitus can result from prolonged GH abuse (pmc.ncbi.nlm.nih.gov)(tga.gov.au). Even in lower doses, GH can unmask a tendency toward diabetes; in high doses it almost invariably raises glucose levels. Users often report increased thirst and urination (early signs of impaired glucose tolerance). Furthermore, GH can unfavorably alter lipid profiles (e.g. lower HDL cholesterol) and increase risk of hypertension, compounding cardiovascular risk. High blood pressure may result from both fluid retention and metabolic effects.
Acromegaly-like changes:
Over time, excess GH/IGF-1 can cause growth of certain tissues. Users who abuse GH for extended periods sometimes develop coarse, enlarged facial features (growth of jawbone or brow, widened nose), enlarged hands and feet (ring/glove/shoe sizes may increase), and organ enlargement (GH can cause growth of the heart, liver, intestines, etc.). Enlargement of the heart (cardiomyopathy) is a particularly dangerous outcome, potentially leading to heart failure or arrhythmias. Unlike muscle, which has a limited capacity to grow, internal organs and cartilage can thicken under excess GH – leading to the notorious “GH gut” (protruding abdomen some bodybuilders develop, thought to be due to organomegaly and visceral growth from chronic high doses). These acromegalic changes can be irreversible if GH is abused for years.
Fatigue and reduced fitness:
Although moderate GH can subjectively increase energy, excessive GH can paradoxically worsen exercise capacity – likely due to muscle insulin resistance and metabolic perturbations. Some users report that while they look bigger on GH, their endurance suffers (e.g. get winded more easily). GH can also cause muscle pain (myalgias) and weakness in a dose-dependent manner.
Other side effects:
Headaches and intracranial hypertension can occur (as with therapeutic use, but risk is higher at abuse doses). GH can contribute to sleep apnea by enlarging soft tissues (and acromegaly is known to cause sleep apnea). Profuse sweating and skin changes (oily skin) are also noted. High IGF-1 levels might promote growth of malignancies; there is concern that cancer risk could be increased by GH abuse, given IGF-1’s role in cell proliferation (although data is not clear, it’s a theoretical risk – users with a predisposition to cancers could be accelerating a problem).
In addition to GH’s direct effects, there are practical risks associated with off-label use. Since non-prescription GH is often obtained via the black market, products may be of dubious quality or counterfeit. There have been cases of underground “GH” that was actually something else, or vials contaminated with bacteria or impurities. If a person injects counterfeit or unsterile preparations, they risk infections (such as HIV, hepatitis, or abscesses) and unknown drug effects. Even legitimate GH, if misused with non-sterile technique, can transmit infections when needles are shared. Years ago, some athletes used cadaveric GH (extracted from human pituitaries) which tragically caused Creutzfeldt–Jakob disease in recipients – while that source is obsolete, it underscores the dangers of unsupervised hormone sourcing.
Finally, from a legal and ethical standpoint, using GH for bodybuilding is illegal without a prescription in many countries and banned in sports by anti-doping agencies. Athletes found using it can face sanctions. The cost of GH is also very high, which can lead some to dangerous cost-saving measures (like using insulin or IGF stimulators, or purchasing from unverified suppliers).
In summary, GH abuse can harm multiple organ systems. Documented effects include edema, arthralgias, carpal tunnel syndrome, insulin resistance progressing to diabetes, hypertension, cardiomegaly and heart failure, abnormal growth of bone and organs, and possibly shortened lifespan from these complications. Many of these changes (especially bone and organ growth) are not fully reversible even after stopping GH. For example, acromegaly patients (who essentially experience chronic GH excess from a tumor) suffer elevated rates of arthritis, diabetes, and heart disease leading to premature mortality. It is reasonable to expect that a healthy person who artificially induces an acromegaly-like state with excess GH could face similar outcomes if they continue long-term. Even shorter cycles of GH can cause bothersome temporary side effects (like severe bloating and carpal tunnel symptoms that can interfere with training).
Caveat emptor:
Due to these risks, medical experts strongly advise that human growth hormone only be used under physician supervision for legitimate medical indications . The bodybuilding practices are essentially a large uncontrolled experiment. While some individuals appear to tolerate moderate GH doses and enjoy cosmetic benefits, others have suffered health issues. Moreover, the expected gains in athletic performance are not clearly supported by science – a review in Annals of Internal Medicine concluded that GH did not significantly enhance muscle strength and could decrease endurance, meaning users risk their health for questionable strength benefits. In the end, the pursuit of extreme muscle growth with GH exemplifies “too much of a good thing can be bad”: growth hormone is vital for those who lack it, but in excess it can cause disease and dysfunction.
👨⚕️ Author
Dr. Jonathan R. McKenna, MD, FACE, Endocrinology & Metabolic Medicine
Credentials:
Board-Certified Endocrinologist (American Board of Internal Medicine)
Fellow of the American College of Endocrinology (FACE)
M.D. – Mayo Clinic Alix School of Medicine, Rochester, MN
Residency – Internal Medicine, Cleveland Clinic
Fellowship – Endocrinology, Stanford University Medical Center
Expertise:
Dr. Jonathan R. McKenna is a U.S.-based endocrinologist specializing in adult and pediatric growth hormone disorders, hormone-replacement therapy, and clinical pharmacology of recombinant biologics. He has served as a principal investigator in multiple FDA-regulated trials evaluating the efficacy and safety of somatropin formulations, including Saizen®, Genotropin®, and Norditropin®.
Editorial & Research Background:
Contributor to the Journal of Clinical Endocrinology & Metabolism and Endocrine Reviews
Former consultant for the Endocrine Society’s guideline committee on adult GH deficiency
Regular speaker at the American Association of Clinical Endocrinology (AACE) annual congress
Author Statement:
Dr. McKenna’s analyses combine evidence-based endocrinology with clinical pharmacology to help readers understand not only how somatropin is used medically, but also the risks of its misuse in non-therapeutic contexts such as bodybuilding.
Frequently Asked Questions About Saizen 8.8 mg
How many IU are in Saizen 8.8 mg?
Each vial of Saizen 8.8 mg contains approximately 26.4 IU of recombinant human growth hormone (somatropin). One milligram of Saizen equals roughly 3 IU, which is the standard conversion used for growth hormone dosing.
How to reconstitute Saizen 8.8 mg correctly?
To prepare Saizen 8.8 mg for injection, mix the lyophilized powder with 2 to 3 mL of Bacteriostatic Water for Injection (0.9% benzyl alcohol). Direct the liquid against the wall of the vial and swirl gently until fully dissolved. The solution should be clear and free of particles. Do not shake the vial, as this can damage the hormone structure.
How long Saizen 8.8 mg remains stable after reconstitution?
Once reconstituted with bacteriostatic water, Saizen 8.8 mg remains stable for up to 14 days when stored in a refrigerator between 2–8 °C (36–46 °F). If mixed with sterile water instead, the solution must be used immediately because it lacks preservatives and cannot be stored.
What are the recommended doses of Saizen 8.8 mg for children and adults?
In pediatric growth hormone deficiency, the typical Saizen 8.8 mg dosage is about 0.18 mg per kilogram of body weight per week, which equals roughly 0.54 IU/kg/week, divided into daily injections.
In adults with confirmed growth hormone deficiency, treatment usually starts at 0.2 mg per day (about 0.6 IU/day) and increases gradually every few weeks to maintain IGF-1 levels within the normal range for the patient’s age.
Where to inject Saizen 8.8 mg?
Saizen 8.8 mg is administered by subcutaneous injection into areas with subcutaneous fat such as the thigh, abdomen, upper arm, or buttocks. Injection sites should be rotated regularly to prevent irritation, swelling, or lipoatrophy at the same location.
Can healthy adults use Saizen 8.8 mg for bodybuilding or anti-aging?
Saizen 8.8 mg should not be used by healthy adults for bodybuilding, fat loss, or anti-aging purposes. Off-label use of somatropin at high doses increases the risk of adverse effects such as edema, joint pain, insulin resistance, diabetes, and abnormal organ growth. Saizen therapy must always be prescribed and monitored by a qualified endocrinologist for approved medical indications only.
📚 References (APA 7th Edition)
U.S. Food and Drug Administration (FDA). (2007). Saizen® (somatropin [rDNA origin]) for injection — Full Prescribing Information. EMD Serono, Inc. Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/019764s035lbl.pdf
EMD Serono, Inc. (2023). Saizen® somatropin [rDNA origin] for injection — Professional Information. Retrieved from https://www.emdserono.com/us-en/pi/saizen-ce-pi.pdf
Drugs.com. (2024). Saizen (somatropin) — Uses, Dosage, Side Effects & Warnings. Retrieved from https://www.drugs.com/pro/saizen.html
PDR.net (Physicians’ Desk Reference). (2024). Saizen — Somatropin (rDNA origin): Drug Summary. Retrieved from https://www.pdr.net/drug-summary/Saizen-somatropin–rDNA-origin–1170
Merck KGaA / EMD Serono. (2022). Saizen Click.Easy® Product Monograph — Lyophilized powder for injection 8.8 mg. Darmstadt, Germany: Merck KGaA.
Ho, K. K. Y., & Participants of the GH Deficiency Consensus Workshop. (2007). Consensus guidelines for the diagnosis and treatment of adults with growth hormone deficiency: Summary statement of the Growth Hormone Research Society Workshop. Journal of Clinical Endocrinology & Metabolism, 92(11), 3950–3957. https://doi.org/10.1210/jc.2007-0111
Molitch, M. E., Clemmons, D. R., Malozowski, S., Merriam, G. R., Shalet, S. M., & Vance, M. L. (2011). Evaluation and treatment of adult growth hormone deficiency: An Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 96(6), 1587–1609. https://doi.org/10.1210/jc.2011-0179
Liu, H., Bravata, D. M., Olkin, I., Friedlander, A., Liu, V., Roberts, B., & Hoffman, A. R. (2008). Systematic review: The safety and efficacy of growth hormone in the healthy elderly and in athletes. Annals of Internal Medicine, 148(10), 747–758. https://doi.org/10.7326/0003-4819-148-10-200805200-00218
Holt, R. I. G., & Sonksen, P. H. (2008). Growth hormone, IGF-I and insulin and their abuse in sport. British Journal of Pharmacology, 154(3), 542–556. https://doi.org/10.1038/bjp.2008.110
Deyssig, R., Frisch, H., Blum, W. F., & Waldhör, T. (1993). Effect of growth hormone treatment on anabolic steroid–induced muscle hypertrophy in strength-trained athletes. Clinical Endocrinology, 38(1), 15–20. https://doi.org/10.1111/j.1365-2265.1993.tb00962.x
Saugy, M., Robinson, N., Saudan, C., Baume, N., Avois, L., & Mangin, P. (2006). Human growth hormone doping in sport. British Journal of Sports Medicine, 40(Supplement 1), i35–i39. https://doi.org/10.1136/bjsm.2006.027573
Birzniece, V., Nelson, A. E., & Ho, K. K. Y. (2011). Growth hormone and physical performance: Physiology, pharmacology, and abuse. Endocrine Reviews, 32(2), 102–132. https://doi.org/10.1210/er.2010-0009
Mayo Clinic. (2024). Somatropin (injection route): Description and precautions. Retrieved from https://www.mayoclinic.org/drugs-supplements/somatropin-injection-route/description/drg-20070877
Healthy.Kaiser Permanente. (2024). Saizen 8.8 mg subcutaneous solution: Drug encyclopedia. Retrieved from https://healthy.kaiserpermanente.org/health-wellness/drug-encyclopedia/drug.saizen-8-8-mg-subcutaneous-solution.183447
Ocean Breeze Healthcare. (2024). Saizen 8.8 mg (somatropin) product overview and storage information. Retrieved from https://www.oceanbreezehealthcare.com/saizen
Related products
210 ui – Genli Pharmaceuticals Domestic USA
$280.00Add to cartPharmacological action. In vitro, preclinical, and clinical trials have shown that Gentropin lyophilized powder is a therapeutic equivalent to human pituitary-derived growth hormone and achieves pharmacokinetic profiles similar to normal adults.
Espirol (Clenbuterol ) 25mcg 100 tabs – Medical Pharma
$69.00Add to cartClenbutérol, chlorhydrate de; Clenbuteroli hydrochloridum; Hidrocloruro de clenbuterol; Klenbuterol hydrochlorid; Klenbuterolhidroklorid; Klenbuterolhydroklorid; Klenbuterolihydrokloridi; Klenbuterolio hidrochloridas; NAB-365 (clenbuterol). 1-(4-Amino-3,5-dichlorophenyl)-2-tert-butylaminoethanol hydrochloride.
Phentermine 15mg 30 tabs – Acxion Buying Steroids
$77.00Add to cartDiet and exercise are the keys to losing weight. The concept of ‘diet’ was popularized (or at least attributed to it) by the poet Lord Byron, an icon of British romanticism who ate slices of bread, tea and potatoes with vinegar, with the sole purpose of maintaining his pale and thin appearance.
Since then, the keys to voluntary weight loss have been discovered, based on the fact that the number of calories we eat must be less than those we consume in our daily activities. Increasing physical effort increases what we spend, and eating less reduces what we have available to consume. Although with the advancement of scientific research, other factors that affect weight loss have been discovered (such as metabolic rate, age, sleep…), diet and exercise are the cornerstones.







