Most Popular steroids USA
-
 Trenbolone 200 20ml - Sydgroup
$53.00
Trenbolone 200 20ml - Sydgroup
$53.00 -
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
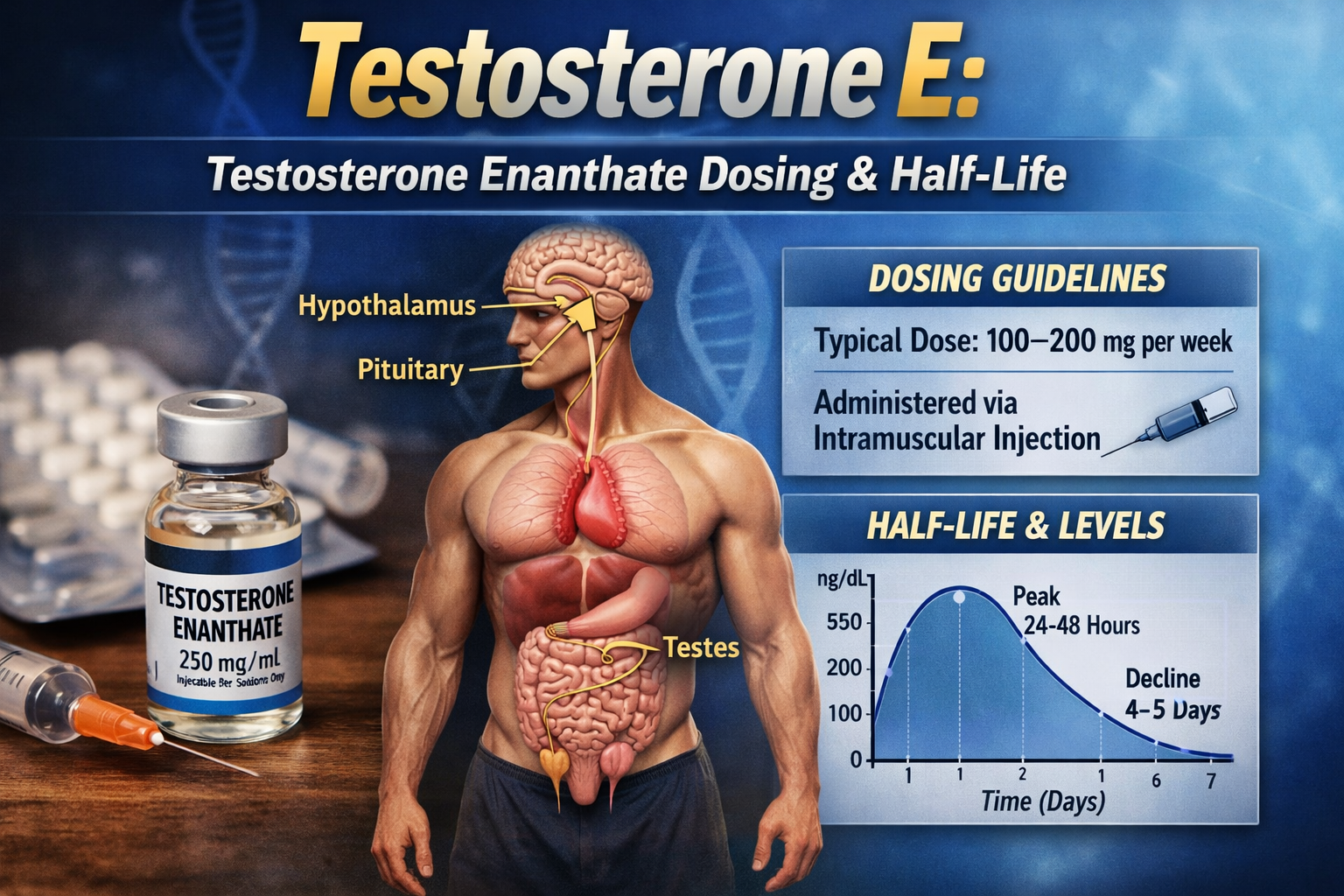
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.












Free Testosterone
News Author: Laurie Barclay, MD
May 23, 2003 — Serum free testosterone is inversely related to carotid intima-media thickness (IMT) and plaque score (PS), according to the results of a study published in the June issue of Diabetes Care. Prospective intervention trials are long overdue, the editorialist suggests.
“Male sex is an independent risk factor for cardiovascular disease (CVD),” write Michiaki Fukui, MD, from Osaka General Hospital in Japan, and colleagues. “There is evidence to suggest that low concentrations of testosterone are associated with an increased risk of CVD in men.”
Of 253 consecutive men with type 2 diabetes, 154 underwent carotid ultrasound. Free testosterone was inversely correlated with IMT (r = -.206; P = .0103), with PS (r = – .334; P < .001), and with age (r = – .420; P < .0001), and it was positively correlated with total cholesterol (r = .145; P = .0238)
“Large prospective trials and intervention studies are needed to better assess the metabolic and cardiovascular benefits of testosterone,” the authors write.
In an accompanying editorial, Shalender Bhasin, MD, and Karen Herbst, MD, PhD, from Charles R. Drew University of Medicine and Science in Los Angeles, California, review the effects of testosterone in animal models and in clinical studies of atherosclerosis, and they agree with the need for prospective, long-term, placebo- controlled, randomized clinical trials.
“The available data suggest that serum testosterone levels in the range that is mid- normal for healthy young men are consistent with an optimal cardiovascular risk profile at any age, and that testosterone concentrations either above or below the physiologic male range may increase the risk of atherosclerotic heart disease,” they write. “Prescription sales of testosterone products have been increasing at an alarming rate…. These trends in testosterone sales are of great concern because the long-term risks and benefits of testosterone replacement in older men are largely unknown.”
Dr. Bhasin has financial arrangements with Solvay, Kellegy, ALZA, DTG, and TheraTech.
Diabetes Care. 2003;26:1869-1873
Learning Objectives
Upon completion of this activity, participants will be able to:
⦁ Explain the controversy over the effect of androgenic steroids, whether intrinsic or externally administered, on plasma lipid levels and atherosclerosis in men.
⦁ Describe the results of research studying the association between serum free testosterone concentration and carotid atherosclerosis in men with type 2 diabetes.
Clinical Context
According to editorialists Bhasin and Herbst, there is a widespread misperception that the sex differences in the prevalence of coronary artery disease (CAD) are due to higher testosterone concentrations in men and that testosterone supplementation in men would adversely affect the plasma lipoprotein profile, therefore increasing the risk of atherosclerotic heart disease.
Case reports of cardiovascular accidents among athletes who had abused androgenic steroids have strengthened this notion; however, there are no data substantiating a cause-and-effect relationship between androgens and cardiovascular disease.
Because there are currently no intervention studies on the effects of long-term testosterone administration on CAD, inferences about the risks of testosterone administration have been derived from studies assessing the effect of testosterone on lipoprotein metabolism, markers of inflammation, and insulin sensitivity.

Although larger than physiologic doses of testosterone and dihydrotestosterone (DHT) undoubtedly decrease plasma high-density lipoprotein (HDL) cholesterol levels, physiologic testosterone replacement in older men has been associated with only a modest decrease or no decrease in plasma HDL cholesterol. Cross-sectional studies of middle-aged men find a direct, rather than inverse, relationship between serum testosterone levels and plasma HDL cholesterol concentrations. Testosterone administration to men has very little effect on total cholesterol, triglyceride, and overall low-density lipoprotein (LDL) levels, but it does decrease LDL particle size.
As men age, their testosterone levels decline and fat mass increases. Serum testosterone levels are correlated inversely with fat mass, particularly visceral fat. Testosterone replacement in young and older hypogonadal men is associated with a reduction in overall fat mass and inhibition of uptake of labeled triglycerides and enhanced lipid mobilization in visceral fat.
Marin and colleagues, writing in the December 1992 issue of the International Journal of Obesity and Related Metabolic Disorders, reported that testosterone supplementation of middle-aged men with truncal obesity and low-normal testosterone levels is associated with a reduction in visceral fat volume, serum glucose concentration, blood pressure, and an improvement in insulin sensitivity, suggesting that testosterone is an important regulator of regional fat metabolism.
The available data suggest that serum testosterone levels in the range that is mid-normal for healthy young men are consistent with an optimal cardiovascular risk profile at any age, and that testosterone concentrations either above or below the physiologic male range may increase the risk of atherosclerotic heart disease. The effects of testosterone replacement on cardiovascular risk in humans have never been directly examined.
Testosterone tends to bind with sex hormone binding globulin (SHBG). But some testosterone remains freely circulating in the bloodstream. Total testosterone is a measure of both free and SHBG-bound forms of the hormone.
The aim of this study was to evaluate the relationship between serum testosterone concentration, and, in particular, free (unbound) testosterone concentration, and carotid atherosclerosis as well as major cardiovascular risk factors in men with type 2 diabetes.
Study Highlights
Serum free and total testosterone concentrations were measured in 253 consecutive men with type 2 diabetes. The relationship between serum testosterone concentration and carotid atherosclerosis, determined by ultrasonographically evaluated IMT and PS, in a subgroup of 154 diabetic patients was evaluated.
Inverse correlations were found between free testosterone concentrations and IMT and between free testosterone concentrations and PS.
The IMT and PS were significantly greater in patients with lower concentrations of free testosterone than in patients with higher concentrations of free testosterone. An inverse correlation was found between serum free testosterone concentration and age.
A positive correlation was found between serum free testosterone and total cholesterol concentrations.
Pearls for Practice
Serum total testosterone concentrations are not significantly different between patients with or without CVD. However, serum free testosterone concentrations were significantly inversely correlated with ultrasonographically evaluated mean IMT and PS, which are early preclinical markers of atherosclerosis.
Serum free testosterone concentration correlated with the severity of atherosclerosis, regardless of the presence of clinical manifestations.
Post Test
- According to editorialists Bhasin and Herbst, which of the following statements is FALSE?
a. Testosterone supplementation in men adversely affects the plasma lipoprotein profile, therefore increasing the risk of atherosclerotic heart disease
b. Serum testosterone levels in the range that is mid-normal for healthy young men are consistent with an optimal cardiovascular risk profile at any age
c. Testosterone administration to men has very little effect on total cholesterol, triglyceride, and overall LDL levels, but it does decrease LDL particle size
d. Larger than physiologic doses of testosterone and DHT decrease plasma HDL cholesterol levels. - According to the current study, which of the following statements is true?
a. There is a direct correlation between free testosterone concentration and IMT (ie, the higher the free testosterone, the thicker the intima-media)
b. There is a direct correlation between free testosterone concentration and PS (ie, the higher the free testosterone, the higher the PS)
c. Serum total testosterone concentrations are not significantly different between patients with or without CVD
d. A direct correlation was found between serum free testosterone concentration and age