Most Popular steroids USA
-
 Trenbolone 200 20ml - Sydgroup
$53.00
Trenbolone 200 20ml - Sydgroup
$53.00 -
Primobolan for sale 100mg 10 ml Human Pharma in USA
$115.00
-
NPP Steroid 100mg 10 ml Premium Domestic USA
Original price was: $99.00.$80.00Current price is: $80.00.
-
Anavar for Sale in USA – 10mg 80 Tabs GPH-Premium
Original price was: $110.00.$80.00Current price is: $80.00.
-
Buy Anavar 10mg – Purchase Geno Pharma
$99.00
-
Testosterone Cypionate Buy 300mg 10ml Geno Pharma
$99.00
-
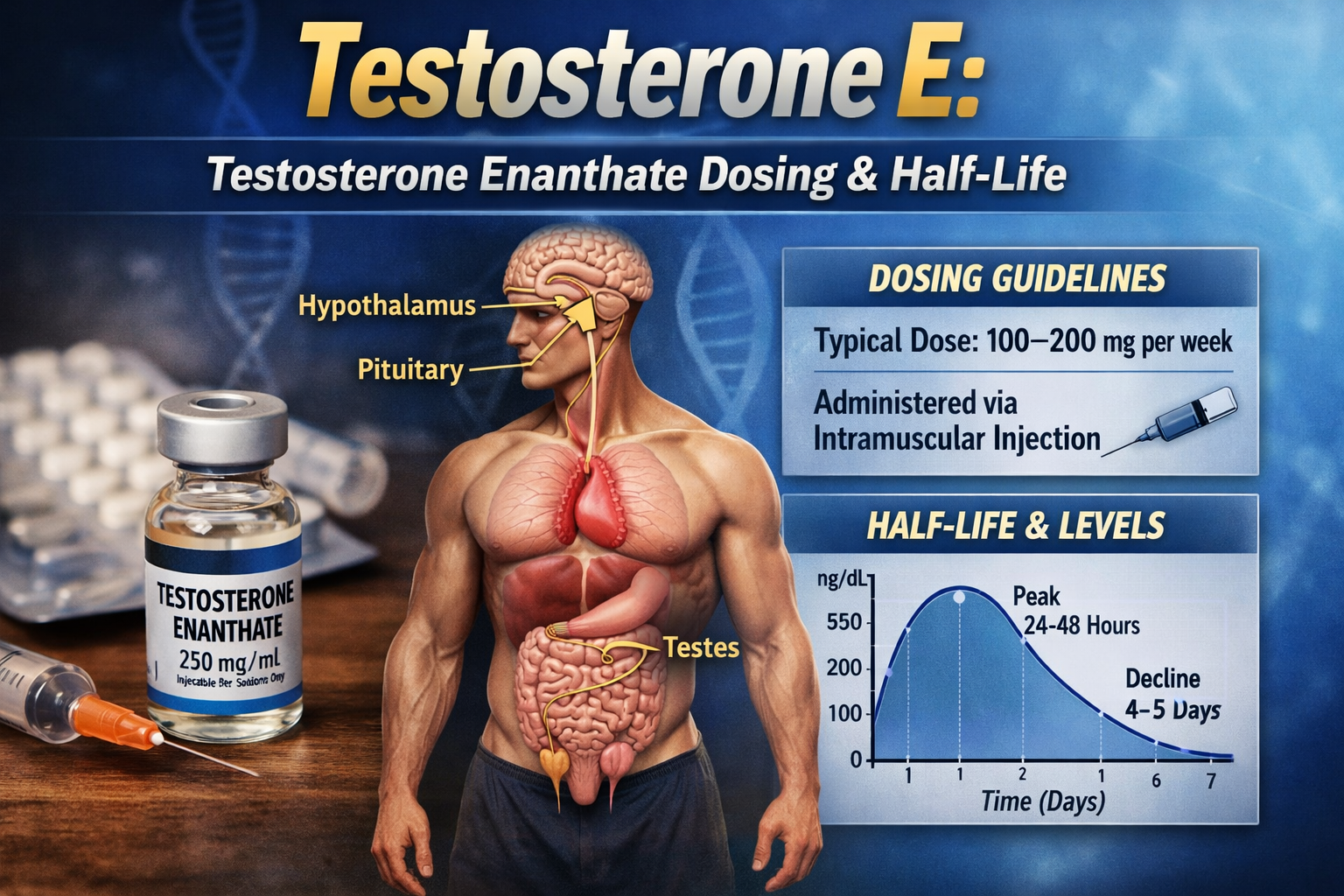
Buy Testosterone E 300mg 10 ml Geno Pharma Domestic USA/CA
$99.00
-
Testosterone Cypionate 200 Biopharma 10 amp
Original price was: $99.00.$72.00Current price is: $72.00.
-
Testosterone 400 Biopharma 10 Ampoules
Original price was: $99.00.$75.00Current price is: $75.00.
-
Eq 300 steroid Rotterdam 10ml
Original price was: $79.00.$69.00Current price is: $69.00.
-
Steroid Deca Geno Pharma 300mg 10ml
Original price was: $110.00.$99.00Current price is: $99.00.
-
Boldenone Cypionate 200 mg / 10 mL Geno Pharma
Original price was: $90.00.$85.00Current price is: $85.00.











Anabolic steroid aromatization
You most probably have heard that some anabolic steroids aromatize in the body, but which ones do so and why they do that?
For this we have to review the testosterone metabolism in the body.
Androgens are the precursors of all steroid hormones (with the exception of progestins), therefore androgens are needed in males and females, and produced in different organs (testis, ovaries and adrenal glands).
The major androgen in men is testosterone (the most potent androgen), produced in the testis, it acts either directly in androgenic receptors or after being converted to dihydrotestosterone (DHT); Other major circulating androgens in men include androstenedione, androstenediol, dehydroepiandrosterone (DHEA) and dehydroepiandrosterone sulfate (DHEA-S). [1]
Several steps are needed for androgen production, beginning with cholesterol, this is represented in the next figure:
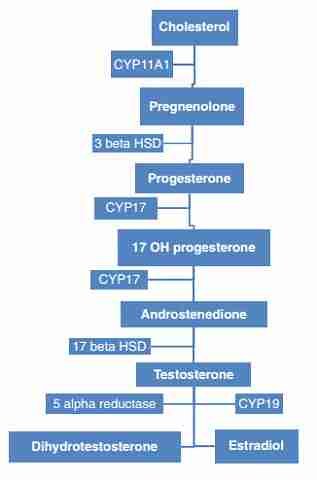
As you can see, the steps are: cholesterol > pregnenolone > progesterone > 17-OH progesterone > androstenedione > testosterone
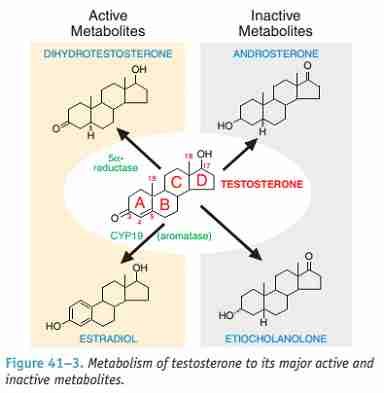
Once in this step, the available testosterone will be metabolized either by 5 alpha reductase hormone (making dihydrotestosterone) or by aromatase (CYP19) making estradiol (aromatization), as shown in the next figure

About 85% of estrogens circulating in men are made in extra-gonadal sites (adipose tissue mainly), the remainder 15% is made by the gonads (testis)
The conversion will be directly related to the substrate available, meaning that, the more testosterone available in the adipose tissue (fat tissue) the more conversion will take place, and this is completely reasonable as estrogens serve many purposes in men, being essential for our physiology.
Being this a conversion of androgens, the more androgenic a substance is, the more aromatization will take place (and more estrogenic production therefore)
With structural modifications to testosterone, the anabolic effects of androgens can be enhanced but, even so, these cannot be divorced entirely from their androgenic effects. Hence, a more accurate term for anabolic steroids is anabolic–androgenic steroids. [2]
This will cause users of anabolic androgenic steroids to have high circulating estrogen levels, even typical levels of women during a normal menstrual cycle; this can cause breast pain and gynecomastia (which is often irreversible) and may be present in 10-34% of users according to a 2004 paper. [3]
Some anabolic steroids are considered to be not aromatized and therefore will not increase estrogen levels, these are:
⦁ Oxandrolone (Anavar)
⦁ Dihydrotestosterone
⦁ Trenbolone
⦁ Fluoxymesterone (Halotestin)
⦁ Drostanolone
⦁ Methyltrienolone (metribolone)
⦁ Furazabol
⦁ Turinabol
⦁ Methenolone
⦁ Mesterolone
⦁ Stanozolol
None of this anabolic steroids are substrate of the aromatase enzyme (meaning it cannot bind this agents) so these will not have any estrogenic effect in the body.
Finally, some agents are considered to be highly estrogenic, like:
⦁ Oxymetholone (anadrol)
⦁ Mibolerone
⦁ Methyltestosterone
⦁ Bolasterone
⦁ Norethandrolone
With these agents, high estrogenic activity must be expected and aromatase inhibitors or anti-estrogenic agents should be used.
Bibliography
1-. The Reproductive System at a Glance. 4th Edition by Linda J. Heffner, Danny J. Schust
2-. Br J Pharmacol. 2008 Jun; 154(3): 502–521. Pharmacology of anabolic steroids. A T Kicman
(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2439524/ )
3-. Regul Toxicol Pharmacol. 2010 Jun;57(1):117-23. doi: 10.1016/j.yrtph.2010.02.001. Epub 2010 Feb 12. Adverse health effects of anabolic-androgenic steroids. van Amsterdam J, Opperhuizen A, Hartgens F.
(http://www.ncbi.nlm.nih.gov/pubmed/20153798 )